간초음파 어떻게 하면 잘 할 수 있을까? 임상의를 위한 실전적 가이드
Abstract
Liver ultrasound is important for screening of hepatocellular carcinoma, hepatitis virus associated chronic hepatitis, and cirrhosis. It is also useful for diagnosis and follow-up of diffuse and focal liver diseases. Liver ultrasound is noninvasive and has no risk of radiation, so we can safely apply it on children and pregnant women. In this article, we discuss how to perform liver ultrasound for better imaging. The liver is the largest organ in abdomen, difficult to examine by one image on a screen, so it is essential that the examiner scan liver systemically. For a better examination, we should keep in mind the followings: 1) Overnight fasting or fasting for 6 hours is necessary prior to an examination. 2) Use a convex probe (2-5 MHz) and, if needed, a linear probe (7-12 MHz). 3) Couinaud’s 8-segment anatomy is useful for localizing hepatic lesions. 4) Subcostal, intercostal, longitudinal, and transverse scans are necessary for each segment and vascular structures. 5) It is necessary to understand characteristic ultrasound findings of benign and malignant tumors when a lesion mass is found. 6) If ultrasound examination is done incompletely due to bowel gas or severe obesity, consider abdominal CT or MRI for further evaluation. 7) Changing the patient’s position is sometimes necessary.
Keywords: Liver; Ultrasonography; Diagnostic imaging
중심 단어: 간; 초음파; 진단적 이미지
서 론
간초음파검사는 간기능 이상의 평가, 미만성 및 국소성 간질환의 진단 및 추적 관찰에 아주 유용한 검사이다[ 1- 3]. 또한 비침습적이고 방사능의 해가 없어 소아나 임산부에서도 안전하게 검사할 수 있다는 장점이 있다[ 1, 2, 4]. 간초음파검사를 잘 하기 위해서는 다음 여덟 가지 기본 사항을 염두에 두어야 한다: 1) 환자는 최소 6시간 금식을 요한다. 검사하러 올 때 껌을 씹지 않도록 설명하고 담배도 피우지 않도록 이야기한다. 2) 볼록형 탐촉자(2-5 MHz)를 사용하지만 필요에 따라(특히 간의 표면을 볼 때) 고주파의 선형 탐촉자를 사용하기도 한다. 3) 좌측 끝에서 우측 끝까지 관찰하며 적절한 체위 조절도 도움이 된다. 4) Couinaud의 분류에 따라 간을 총 8개의 구역으로 나누어 검사한다. 5) 우늑골하스캔, 우늑간스캔, 횡스캔 및 종스캔 등 다양한 접근법을 잘 활용하여 충분히 검사한다. 6) 양성 및 악성 종양의 특징적 초음파 소견을 미리 숙지하고 있어야 하며, 만성 간염 및 간 경변에 동반된 종양의 경우에는 양성처럼 보여도 다른 추가 검사(computed tomography, CT; magnetic resonance imaging, MRI)를 해보는 것을 권유한다. 7) 병변으로 의심되는 부위가 발견되면, 항상 종스캔 및 횡스캔을 같이하여 실재하는 병변이 맞는지 확인한다. 8) 간실질의 에코, 간표면의 요철 여부, 간의 밝기, 간의 크기, 종양성 병변, 문맥 혈전 등을 관찰한다. 물론 이렇게 열심히 하여도 검사가 힘들 때도 있지만 원칙을 지켜서 천천히 꼼꼼하게 검사하면 초음파 실력이 향상되어 실수도 줄일 수 있을 것으로 사료된다.
본 론
Couinaud의 분류
간은 복강 내에서 가장 큰 장기이므로 한 화면에서 간을 전부 다 관찰하는 것은 불가능하다. 그래서 간을 구역을 나누어 관찰한다. 이에 간내 병변의 위치를 표시할 때 가장 많이 이용되는 방법이 Couinaud의 분류이다( Fig. 1). 간 스캔 시에도 Couinaud의 분류에 따라 간을 구역으로 나누어 스캔한다[ 1- 3, 5]. Couinaud의 분류는 간문맥 및 간정맥을 기초로 간을 8개의 구역으로 나누고 있다. 간문맥은 구역의 중심을 간정맥은 구역의 경계를 주행한다고 생각하면 된다[ 1]. 8개의 구역은 다음과 같이 나눈다: S1 (미상엽, caudate lobe), S2 (좌엽 외측 상구역, left lobe lateral superior segment), S3 (좌엽 외측 하구역, left lobe lateral inferior segment), S4 (좌엽 내측 구역, left lobe medial segment), S5 (우엽 전하구역, right lobe anterior inferior segment), S6 (우엽 후하구역, right lobe posterior inferior segment), S 7 (우엽 후 상구역, r ight l obe p osterior s uperior segment), S8 (우엽 전상구역, right lobe anterior superior segment). 실제 해부에서는 S1이 제일 위쪽, 깊은 곳에 위치하고 시계 방향으로 S2부터 S8까지 위치하고 있으나 초음파검사는 아래에서 위를 보면서 검사하므로, S1이 제일 밑에 보이고 반시계 방향으로 S2, S3, S4, S5, S6, S7, S8 순으로 보인다( Fig. 2). 간의 상부에서는 간정맥을 경계로 S2 (좌간정맥의 외측), S4 (좌간정맥과 중간정맥의 사이), S8 (중간정맥과 우간정맥의 사이), S7 (우간정맥의 후측)로 나뉜다[ 4] ( Fig. 3).
간초음파검사할 때 놓치기 쉬운 부위
간초음파검사할 때 좌측 끝에서 우측 끝까지 꼼꼼하게 관찰해야 하는데 간과하기 쉬운 부위가 3군데 있다[ 1, 3, 4] ( Fig. 4). 1) 간의 첨부(dome)
2) 간의 좌엽 외측 끝부분
3) 간의 우엽의 우하구역의 끝부분
Couinaud의 분류에 의한 간의 구역별 초음파 스캔법
간의 각 구역별 초음파 스캔법에 대해 자세히 알아보면 아래와 같다.
미상엽 스캔(S1)
정맥관삭(ligamentum venosum)과 하대정맥(inferior vena cava)를 지표로 하여 검사한다. 간혹 횡스캔에서는 좌간문맥(left portal vein, LPV)의 제부(umbilical portion)에 가려 잘 안보일 수 있으므로 반드시 종스캔을 같이 하는 것을 권장한다( Figs. 5 and 6). Fig. 6에 나온 72세 여성에서 건강 검진상 발견된 미상엽 낭종이 그 예시다.
좌엽 외측 상구역 및 좌엽 외측 하구역 스캔(S2, S3)
심와부 횡스캔에서 좌간문맥(LPV)의 제부에서 외측으로 분지가 2개 나오는데, 탐촉자에 가까운 것이 S3, 먼 것이 S2이다. 종스캔을 같이 하는 것을 권고하며, 외측으로 탐촉자를 기울여 외측 끝까지 관찰하는 것이 도움이 된다( Fig. 7).
간정맥(hepatic vein) 및 간의 상부 스캔(S2, S4, S7, S8)
좌간정맥(left hepatic vein, LHV)은 간좌엽을 내측과 외측으로 나누고, 중간간정맥(middle hepatic vein, MHV)은 간을 좌엽과 우엽으로 나누며, 우간정맥(right hepatic vein, RHV)은 간우엽을 전구역과 후구역으로 나눈다. 간의 상부에서는 좌간정맥의 외측에 S2, 좌간정맥과 중간간정맥의 사이에 S4, 중간간정맥과 우간정맥사이에 S8, 우간정맥의 뒷쪽에 S7이 위치한다( Fig. 8).
좌엽 내측 구역 스캔(S4)
좌간문맥(LPV)의 제부(umbilical portion)와 횡단부(transverse portion) 및 담낭와(gallbladder fossa)로 둘러싸인 부위로서 여기에서 좌우 간문맥의 연결 부위를 확인할 수 있다( Fig. 9).
간우엽 늑골하스캔(S5, S6, S7)
간우엽 늑골하스캔에서는 S5, S6, S7 구역을 관찰할 수 있다. 간우엽을 늑골하스캔하면 우간문맥(right portal vein, RPV)이 두 갈래로 나누어짐을 볼 수 있는데, 하나는 위쪽으로 분지되고 이것이 S5이며, 하나는 아래쪽으로 분지되고 이는 다시 약간 옆쪽 또는 위쪽으로 분지되는 S6과 아래쪽으로 분지하는 S7이 된다. S8은 늑골하스캔에서는 관찰하기 힘들다( Fig. 10).
우간문맥 포함 간우엽 늑간스캔(S5, S8)
간우엽 늑간스캔하면 담낭 옆에 우간문맥 전분지를 볼 수 있고, 이것이 알파벳 와이(Y) 모양으로 나뉘는데, 탐촉자 쪽(위)으로 가는 것이 S5이고, 탐촉자에서 먼 쪽(옆)으로 가는 것이 S8이다. S8 아래 둥글게 저에코로 보이는 것이 우간정맥이고 그 아래 쪽이 S7이다( Fig. 11).
우간정맥 포함 간우엽 늑간스캔(S5, S6, S7, S8, RHV)
우간문맥 포함 늑간스캔에서 S8 밑에 둥글게 보이는 우간정맥을 탐촉자의 방향을 바꾸어 우간정맥이 길게 나오도록 스캔하면 우간정맥을 중심으로 화면 위쪽은 우측 간엽 전구역(S5, S8), 아래쪽은 우측 간엽 후구역(S6, S7)이 보인다. S5부터 시계 방향으로 S6, S7, S8이 보인다( Fig. 12).
간우엽 하부와 우측 신장 관상면 스캔(간-신장 에코 비교)
전액와선(anterior axillary line) 또는 중액와선(middle axillary line)에서 늑골하종스캔을 하면 간우엽의 후하구역과 우측 신장의 관상면이 관찰된다. 이 스캔법은 간과 신장의 에코 비교에 도움이 되고, 맹점 부위 중 하나인 간우엽의 후하구역의 끝부분을 잘 관찰할 수 있다( Fig. 13).
간의 첨부(dome) 스캔
간 우엽의 늑골하스캔 또는 횡스캔에서 탐촉자를 최대한 눕혀서 호흡을 조절하면서 스캔하면 화면의 아래쪽 횡격막 바로 위쪽에 간의 첨부(dome)가 관찰된다. 간우엽의 늑골하스캔의 경우 환자에게 호흡을 아주 깊게 들이마시게 하고, 배를 불룩하게 내밀도록 하면, 횡격막이 아래쪽으로 내려오고 간도 갈비뼈 아래쪽으로 내려오는 효과가 있어서 간의 첨부 및 전체 간초음파검사에서 좋은 영상을 얻는 데에 도움이 된다. 환자가 깊게 숨을 들이마시는 호흡 조절이 잘 안 되는 경우 간의 첨부는 관찰이 어려울 수도 있다[ 2]. 이 방법으로 간의 첨부가 관찰되지 않으면 우측 옆구리에서 우측 신장의 단축상을 잡아서 탐촉자를 위로 옮기면서 늑간스캔하면 화면의 좌측 상부에 간의 첨부가 보인다( Fig. 14).
간초음파검사에서 관찰할 것들
간실질 에코
정상 간에서는 간실질의 에코가 균일하게 보인다[ 1, 3] ( Fig. 15A). 만성 간염에서는 간실질 에코가 정상이거나 약간 거칠게 보인다( Fig. 15B). 그러나 만성 간염의 정도가 심해지면 간실질 에코가 증가되고 간실질의 거칠어지는 정도가 점차 심해지는데 이런 경우에는 초기 간경변증과 초음파 소견만으로는 감별이 어렵다. 간경변증에서는 간실질 에코가 더 거칠게 보이고 작은 결절이 보일 수 있다[ 1, 2, 6] ( Fig. 15C). 간경변증의 초음파진단에 있어서 간실질의 에코 소견도 중요하지만 간표면의 결절성 변화, 간우엽의 위축과 미상엽과 좌엽의 크기의 증가, 간문맥확장, 비장비대, 부혈관, 복수 등의 초음파 소견을 통해 종합적으로 판단해야 한다[ 1, 2].
간표면의 요철 여부
정상 간은 간표면이 평활하다( Fig. 16A). 만성 B형 간염에서 간표면이 평활하거나 약간 요철이 관찰된다( Fig. 16B, D). 간표면의 요철이 심하거나 간표면이 끊어짐이 관찰되면 간경변증을 의심해봐야 한다( Fig. 16C, E). 간표면의 요철의 존재가 간경변의 조기 진단에 가장 도움이 되는 초음파 소견이다[ 1, 7]. 간표면을 관찰할 때 볼록형 탐촉자로 검사시에는 깊이를 낮추어 표면이 잘 보이도록 화면을 조정하고 필요하면 선형 탐촉자로 간표면을 관찰하는 것이 좋다[ 8] ( Fig. 16D- F).
간의 밝기
정상 간에서는 간의 밝기가 신피질과 비슷하거나 약간 높은 정도이다( Fig. 17A). 지방간에서는 간의 밝기가 신피질보다 많이 높아서 신장의 테두리 고에코가 보이지 않는다( Fig. 17B). 지방간이 심해지면 간문맥의 벽이 잘 안 보이고( Fig. 17C), 더 심해져서 중증 지방간이 되면 초음파의 감쇠가 심해져서 횡격막이 잘 보이지 않는다[ 1- 3, 6, 9] ( Fig. 17D).
간의 크기
간의 크기를 재는 방법은 다양하고 체형에 따라 차이가 있어 신뢰성은 떨어지지만 간의 좌엽과 우엽에서 크기를 측정하여 정상인지 종대되었는지 혹은 위축되었는지 관찰한다. 간좌엽에서는 심와부에서 대동맥이 보이도록 종스캔을 통하여 간의 전후경(anterior-posterior length) ( Fig 18A, a to c)과 두미경(craniocaudal length)을 측정하여( Fig. 18A, a to b) 전후경 5 cm 전후, 두미경 7 cm 전후를 정상 범위로 평가한다. 간우엽에서는 중쇄골선 또는 전액와선에서 간우엽을 종스캔하여 우측 신장 장축과 평행하게 간우엽 하부 끝에서 횡격막까지 측정하거나( Fig. 18B, a to b) 중쇄골선에서 간우엽 늑골하스캔하여 전후경을 측정하게 되며( Fig. 18C, a to b) [ 10], 15 cm 이내를 정상으로 보고, 9 cm 미만이면 위축, 16 cm 이상이면 간종대라고 할 수 있다. 초음파검사에서 간의 크기를 판단하는 데 있어서 절대적인 크기도 의미가 있지만 성별, 신장, 체격에 따라서 변화가 많으므로 상대적인 크기를 고려하여야 하며, 신장, 비장 등 다른 장기와의 비교를 통해서 판단할 수 있어야 한다. 특히 간경변증의 진단에 있어서는 전체 간의 크기보다는 간우엽이 위축되고 간좌엽과 미상엽이 커지는 등의 국소적인 크기 변화를 중심으로 판단해야 한다[ 2].
종괴 존재 여부 및 성상 관찰
세밀하게 관찰하여 간내 종괴가 있으면 놓치지 말아야 하고 종괴가 있으면 크기, 모양, 숫자, 변연의 모양, 내부 에코의 형태 등 종괴의 성상을 포괄적으로 파악해야 한다. 양성 종양으로서 낭종( Fig. 19A), 혈관종( Fig. 19B- D) 등이 의심되는 초음파 소견이 있는지, 아니면 악성 종양으로서 간세포암( Fig. 19E- G), 전이성 간암( Fig. 19H) 등을 시사하는 특징적인 초음파 소견이 있는지를 파악하여야 한다. 초음파 소견만으로 진단이 명확하지 않은 경우에는 반드시 다른 검사(CT, MRI)를 하는 것을 주저하지 말아야 한다. 일반적으로 초음파검사에서 처음 발견된 간내 종양의 경우 단순 간낭종과 같이 분명하게 양성 종양이라는 확신이 서는 경우가 아니라면 복부 전산화단층촬영을 통해서 확인해보는 것이 좋다. 특히 만성 B형 간염이나 간경변증에서는 양성 결절이 의심되어도 복부 전산화단층촬영이나 자기공명영상검사를 해보는 것이 좋다[ 2, 4].
간문맥내 혈전의 존재 여부 및 문맥의 직경이 커졌는지 관찰(Fig. 20)
만성 B형 간염이나 간경변증 환자에서 간실질에 병변이 뚜렷하지 않은데 간문맥내 혈전이 보이는 경우에 이것이 종양(간세포암)에 의한 혈전인지 문맥압 항진에 의한 양성 혈전인지 감별을 요한다. 일반적으로 간세포암에 의한 혈전은 혈전 부위의 문맥직경이 커지고 Color Doppler상 혈전내 혈류가 관찰되고 혈전 주위에 종양이 동반되는 경우가 많다. 정상 간문맥 직경은 13 mm보다 작아야 한다[ 4, 11, 12]. 그 외 조영증강 초음파(contrast enhanced ultrasound)나 탄성 초음파(elastography) 등 특수 초음파를 추가적으로 시행할 수 있다.
보험 규정에 의한 간초음파 스캔법[3]
일반 간초음파
1) 간좌엽 종스캔(S1, S2, S3, ligamentum venosum) ( Fig. 21A) 2) 간좌엽 횡스캔(S1, S2, S3, S4, ligamentum venosum, umbilical portion of LPV) ( Fig. 21B) 4) 간우엽의 횡스캔 또는 늑골하스캔(S5, S6, S7) ( Fig. 21D) 6) 간우엽 하부와 우측 신장 피질 관상면스캔(간과 신장의 에코 비교) ( Fig. 21F)
정밀 간초음파
10) 우간정맥 포함 간우엽 늑간스캔(S5, S6, S7, S8) ( Fig. 21J)
결 론
비침습적인 간초음파검사는 간암의 조기 발견, 간질환의 스크리닝, 미만성 간질환 및 국소성 간질환의 진단 및 추적 관찰에 탁월한 검사법이다. 그러나 검사자의 숙련도에 따라 개개인의 차이가 크기 때문에 기본 검사법에 맞추어 충실하게 검사하지 않으면 병변이 있는데도 놓칠 수 있다. 간초음파검사시 좌측 끝에서 우측 끝까지 구역별로 나누어 꼼꼼하게 관찰할 필요가 있고 간실질 뿐만 아니라 간표면, 혈관 및 담도의 관찰도 필요하다. 간초음파상 종괴가 발견되면 낭종인지, 양성 종양인지 악성종양인지 감별이 필요하고 경우에 따라서는 정확한 진단을 위해서 다른 검사(CT, MRI)의 도움을 받는 것이 좋다. 장관내 가스 등 다른 요인으로 인해 검사가 충분히 이루어지지 못했을 때 환자에게 충분히 설명하고 소견서에 기술하며 간기능 이상이 있거나 증상이 지속되면 다른 검사를 하도록 권유한다.
Figure 1.
Couinaud’s classification. S1, caudate lobe; S2, left lateral superior segment; S3, left lateral inferior segment; S4, left medial segment; S5, right anterior-inferior segment; S6, right posterior-inferior segment; S7, right posterior-superior segment; S8, right anterior-superior segment. 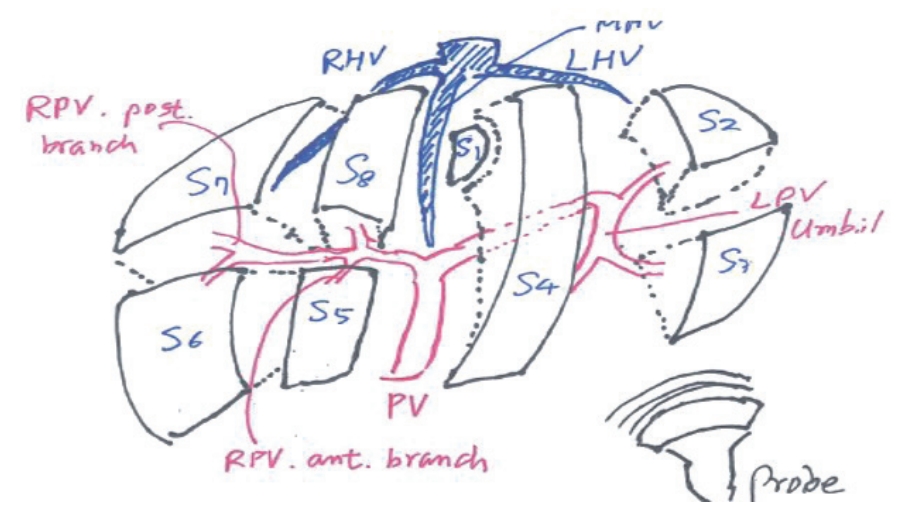
Figure 2.
Ultrasonographic imaging of the liver versus Couinaud’s segmental anatomy. In the real anatomy, S1 is located in the upper posterior portion of the liver. S2 to S8 are located in clockwise sequence. Imaging is obtained from the lower to upper part, therefore S1 is located in the lowest part of the sonographic view. S2 to S8 are located in counterclockwise sequence. 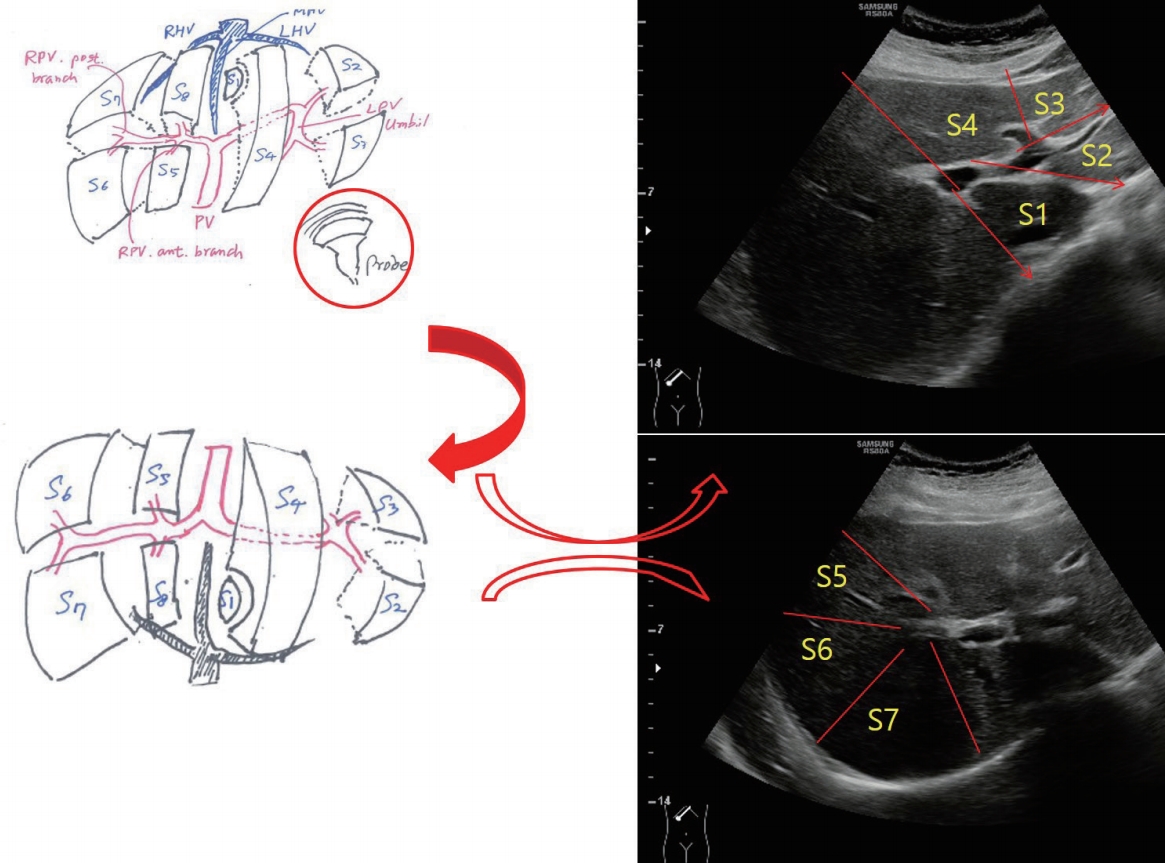
Figure 3.
Segmental anatomy of upper part of liver divided by hepatic vein. S2 is located lateral to the left hepatic vein (LHV), S4 is located between the LHV and the middle hepatic vein (MHV), S8 is located between MHV and right hepatic vein (RHV), and S7 is located medial to the RHV. 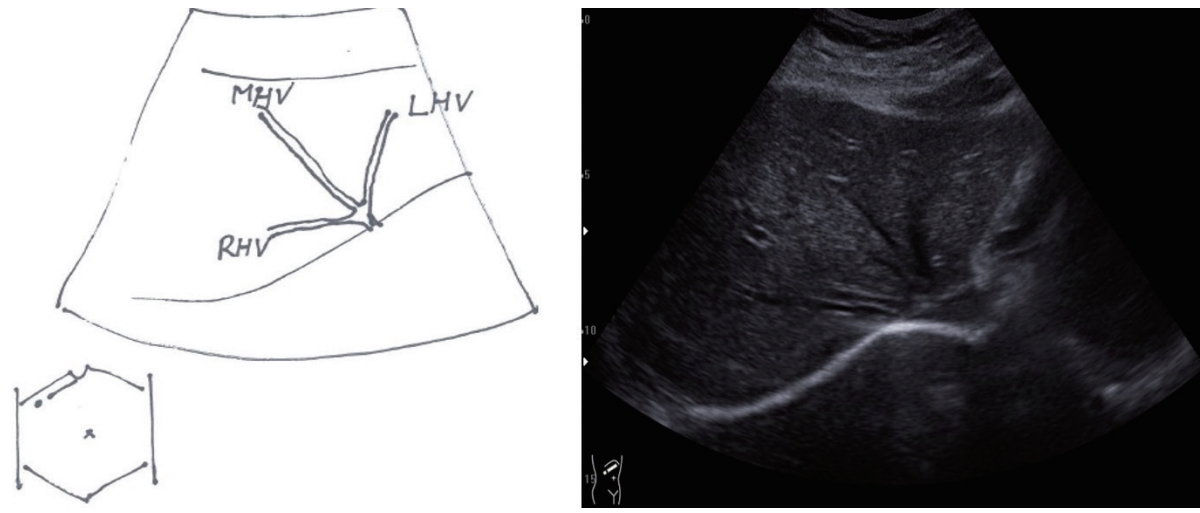
Figure 4.
Blind areas of liver in ultrasound examination. (A) Dome of the liver, (B) the lateral end of the left lobe of the liver, (C) the end of posterior-inferior segment of the right lobe of the liver above right kidney (red circle). 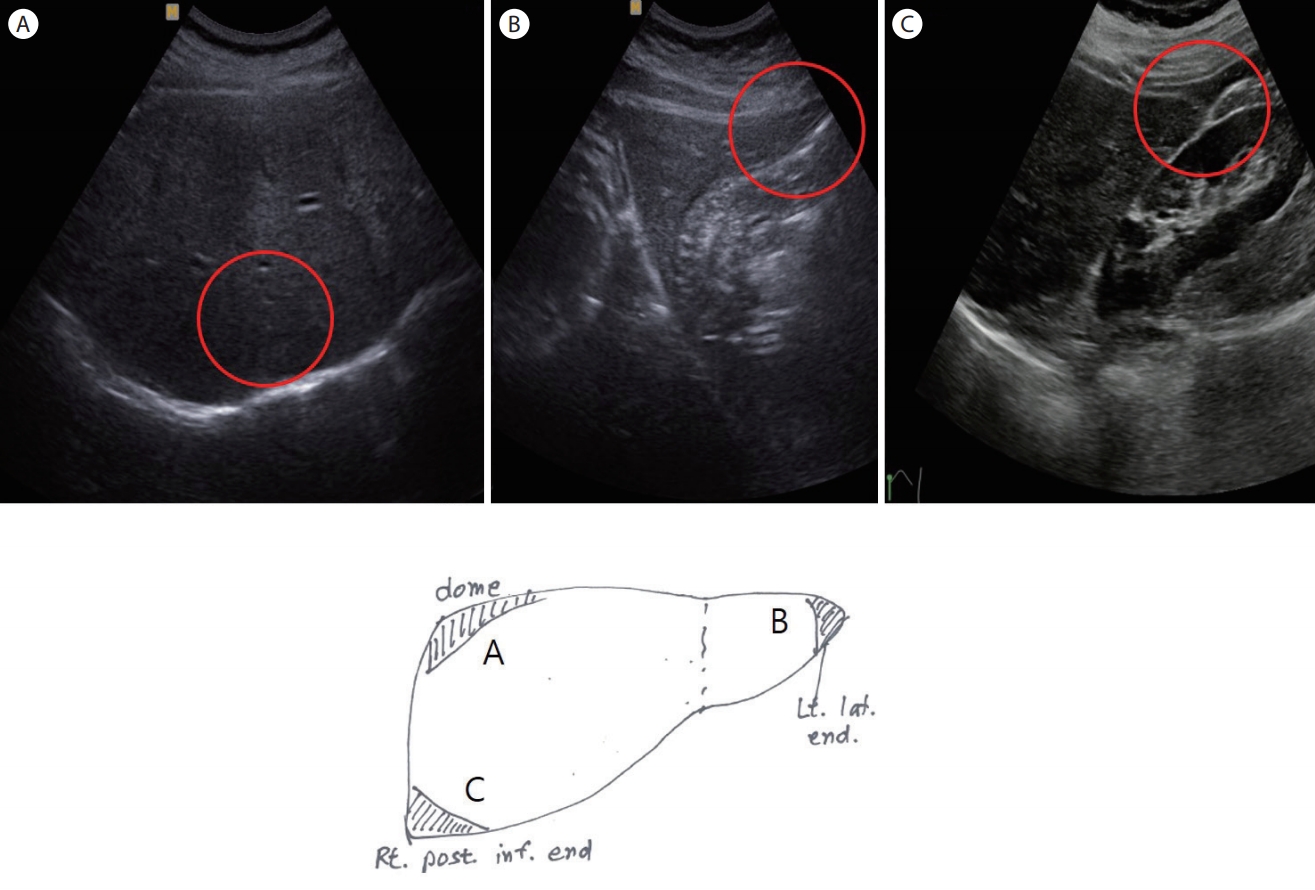
Figure 5.
Caudate lobe (S1). Caudate lobe is located between the ligamentum venosum and the inferior vena cava. Examination of the caudate lobe (S1) is done via transverse and longitudinal scans because the caudate lobe is deep-seated and located above the umbilical portion of left portal vein. A transverse scan of the caudate lobe could be markedly hypoechoic because of masking the umbilical portion of left portal vein. A longitudinal scan of caudate lobe is necessary. IVC, inferior vena cava. 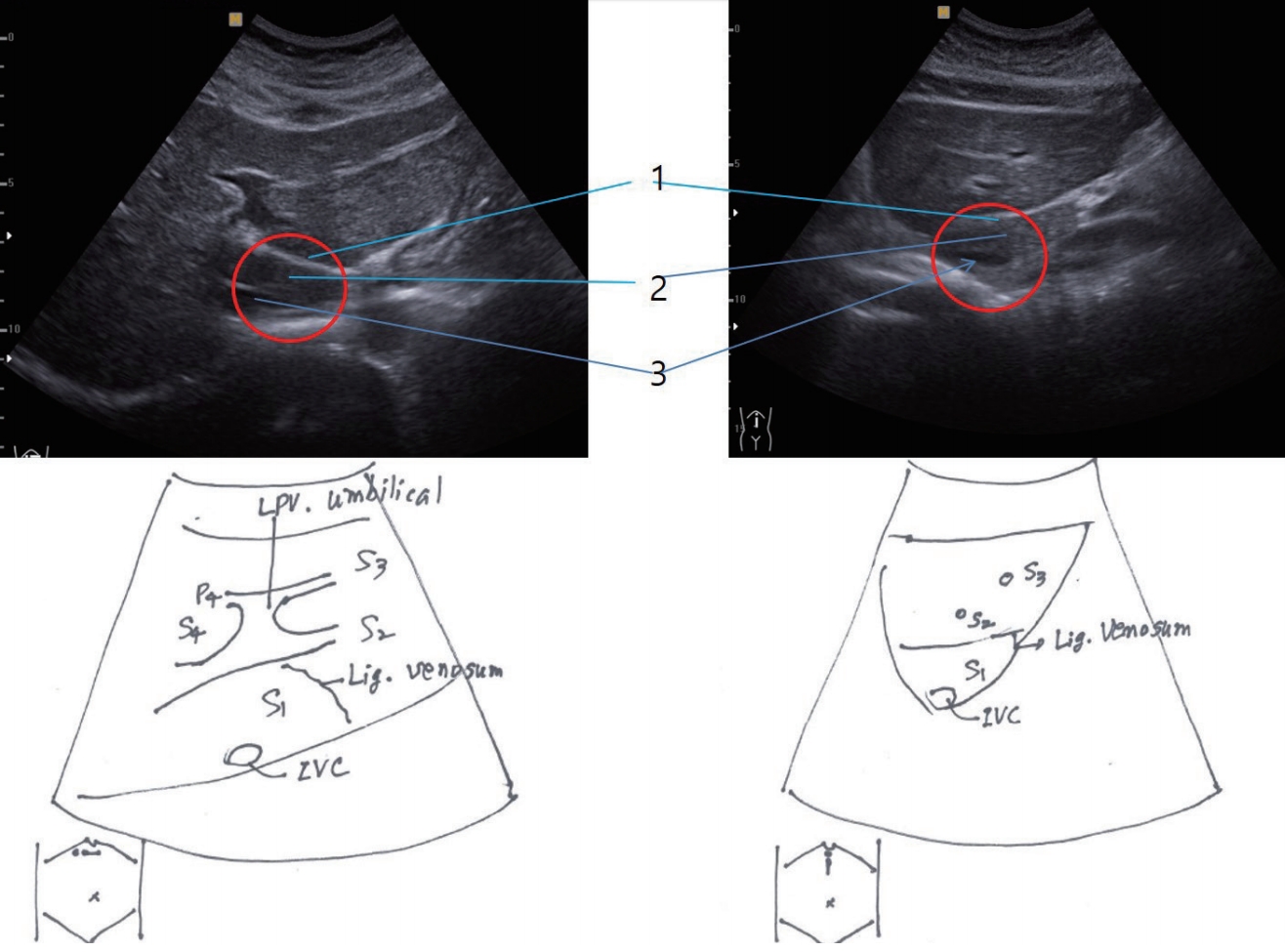
Figure 6.
In a 72-year-old-female, a hepatic cyst was found during her routine check-up. A hypoechoic mass was seen in the caudate lobe in longitudinal and transverse scans (arrowheads). 
Figure 7.
Left lateral superior segment (S2) and left lateral inferior segment (S3). Umbilical portion of the left portal vein (LPV) has two branches laterally. S2 is located far from the probe (lower portion of the image) and S3 is located near the probe (upper portion). ‘1’ indicates S2, ‘2’ indicates S3. 
Figure 8.
Hepatic veins and upper part of liver. The middle hepatic vein (MHV) divides the liver into right and left lobes. The left hepatic vein (LHV) divides the left lobe into medial and lateral segments, and the right hepatic vein (RHV) divides the right lobe into anterior and posterior segments. In the upper part of the liver, S2 is located lateral to the LHV, S4 is located between the LHV and the MHV, S8 is located between the MHV and the RHV, and S7 is located posterior to the RHV. 
Figure 9.
Left medial segment (S4) and portal confluence. S4 is located between the umbilical and transverse portions of the left portal vein and gallbladder (GB) fossa. The portal confluence is also seen in this view. '1' indicates S4, and '2' indicates the portal confluence. 
Figure 10.
Right lobe of liver by right subcostal or transverse scan. The right anterior inferior segment (S5), the right posterior inferior segment (S6) and the right posterior superior segment (S7) are seen in this view. S5 is located laterally and upward, S6 laterally and transverse, and S7 downward (far from the probe). ‘1’ indicates S5; ‘2’, S6; and ‘3’, S7. RPV, right portal vein 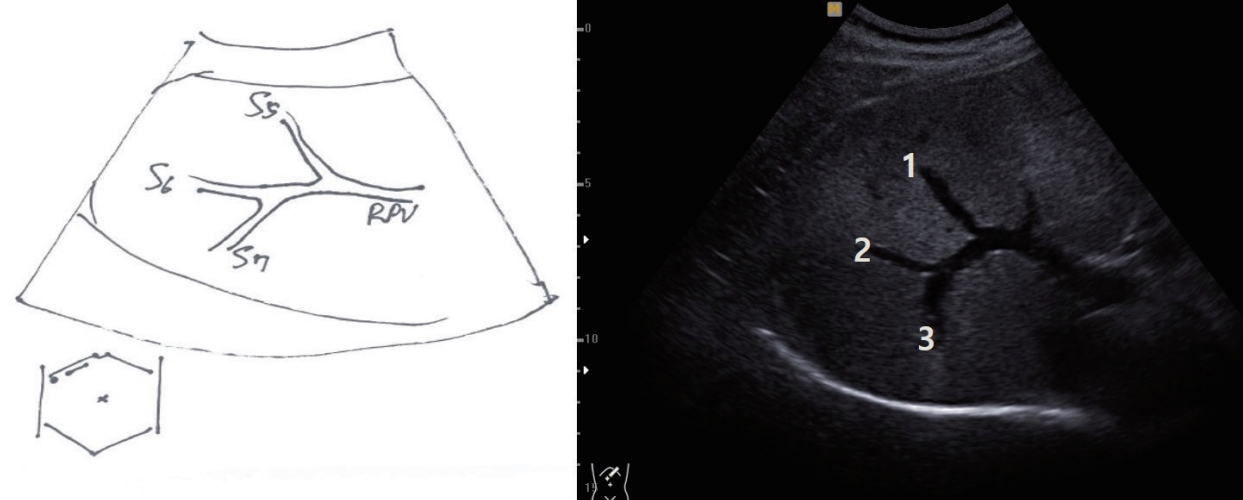
Figure 11.
Right intercostal scan including right portal vein (RPV). In the right intercostal scan, the anterior branch of the RPV is seen near the gallbladder (GB). The RPV branches into a Y-shape. The upward branch (near the probe) supplies the right anterior inferior segment (S5); the other runs laterally or slightly downward, supplying the right anterior superior segment (S8). Below S8, the round, hypoechoic right hepatic vein (RHV) is seen. 
Figure 12.
Right intercostal scan including right hepatic vein (RHV). ‘1’ indicates the right anterior inferior segment (S5); ‘2’, the right posterior inferior segment (S6); ‘3’, the right posterior superior segment (S7); ‘4’, the right anterior superior segment (S8); and ‘5’, the RHV. Scanning of the RHV by changing the angle of the probe reveals an oblique, long RHV between anterior (upper part) and posterior segments (lower part). S5-8 are seen in clockwise sequence. 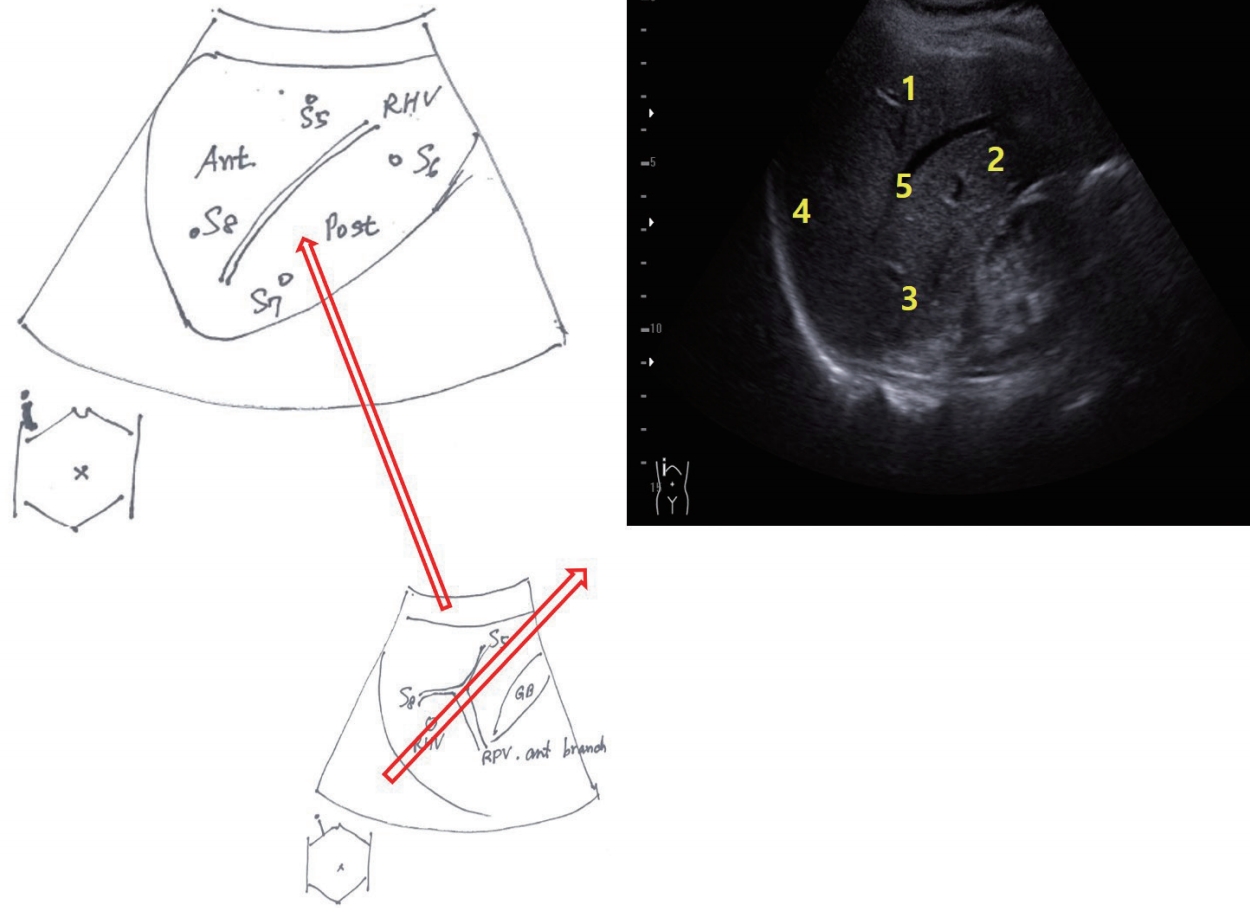
Figure 13.
Scan of right lobe posterior segment and coronal view right kidney. A longitudinal scan in the anterior or middle axillary lines reveals the posterior segment of the right lobe and the coronal view of the right kidney. This scan provides information of differential echogenicity between the liver and the right kidney. We can diagnose a fatty liver with this scan. We also examine the end of the posterior inferior segment of the right lobe above the right kidney, one of the blind areas. 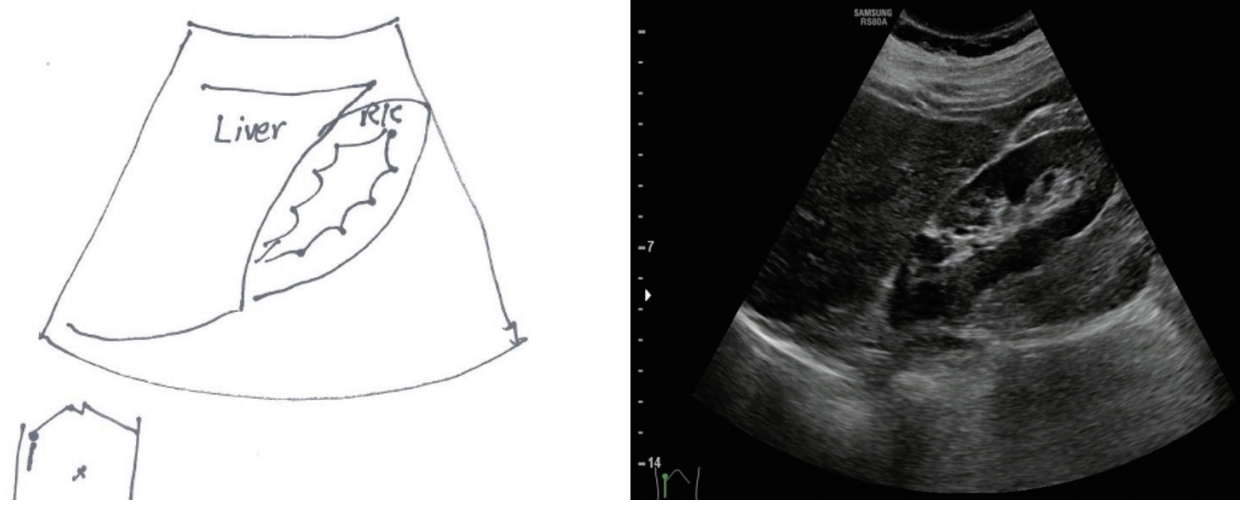
Figure 14.
Scan of dome of liver. The view of the dome of the liver is obtained by the right subcostal or transverse scan with deep inspiration while tilting the probe upwardly. If a subcostal or transverse scan is not available, a right intercostal scan at the right flank with the probe tiling upward shows the dome of liver at the left upper part of the view. ‘1’ and ‘2’ indicate the dome of the liver. 
Figure 15.
Echogenicity of liver parenchyma. (A) Normal liver, (B) chronic hepatitis, (C) liver cirrhosis. Echogenicity of the normal liver is homogenous, but in chronic hepatitis, echogenicity is normal to slightly coarse, and in liver cirrhosis, it is coarse with tiny nodules 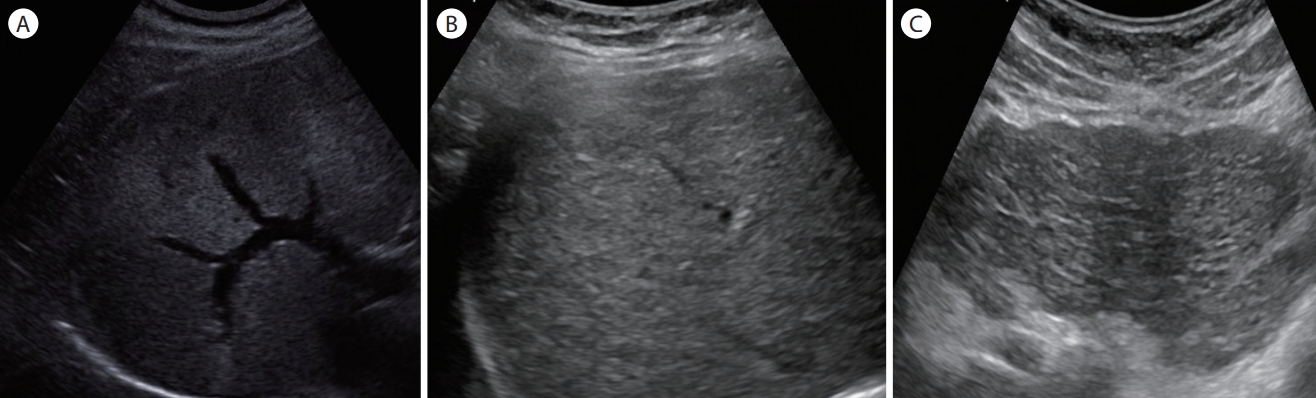
Figure 16.
Surface nodularity of liver. (A) Normal liver, (B) chronic hepatitis, (C) liver cirrhosis, (D) chronic hepatitis, (E) liver cirrhosis, and (F) hepatitis B carrier. The surface of the normal liver is smooth, but in chronic hepatitis, the surface is smooth or slightly notched, and in liver cirrhosis, it is nodular or discontinuous. In some cases of chronic hepatitis B or cirrhosis, examination with a linear probe provides more-accurate information for the surface nodularity and tiny mass lesions near the surface (arrow in F). 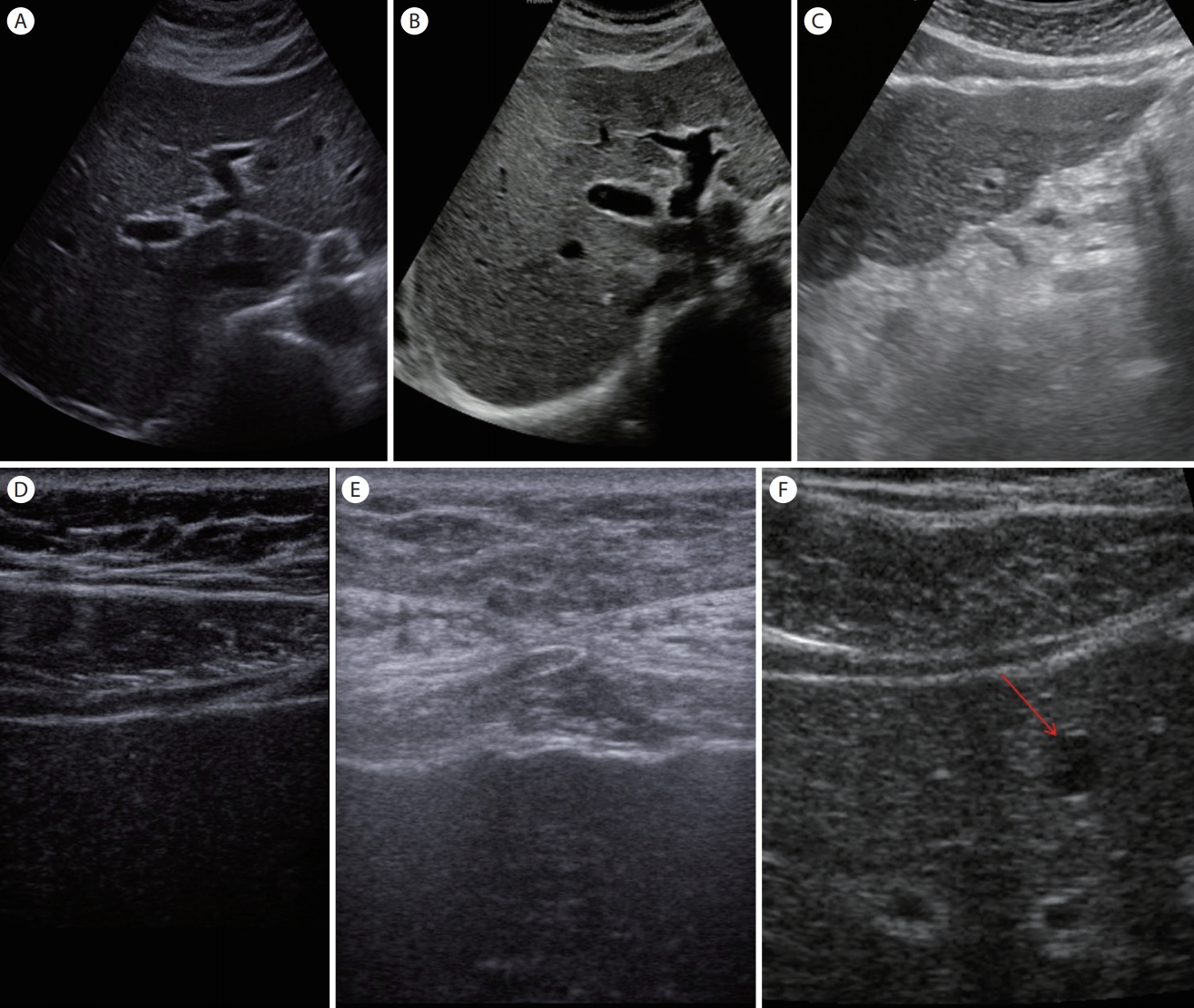
Figure 17.
Brightness of liver. (A) Normal (the brightness of the liver is equal or slightly higher than that of the renal cortex), (B) mild fatty liver (the brightness of the liver is higher than that of the renal cortex, and the portal vein wall is visible). (C) Moderate fatty liver (the brightness of the liver is further increased but the portal vein wall is still discernable). (D) Severe fatty liver (there is poor visualization of the diaphragm due to the deep attenuation of ultrasound and a marked increase in the brightness of the liver). 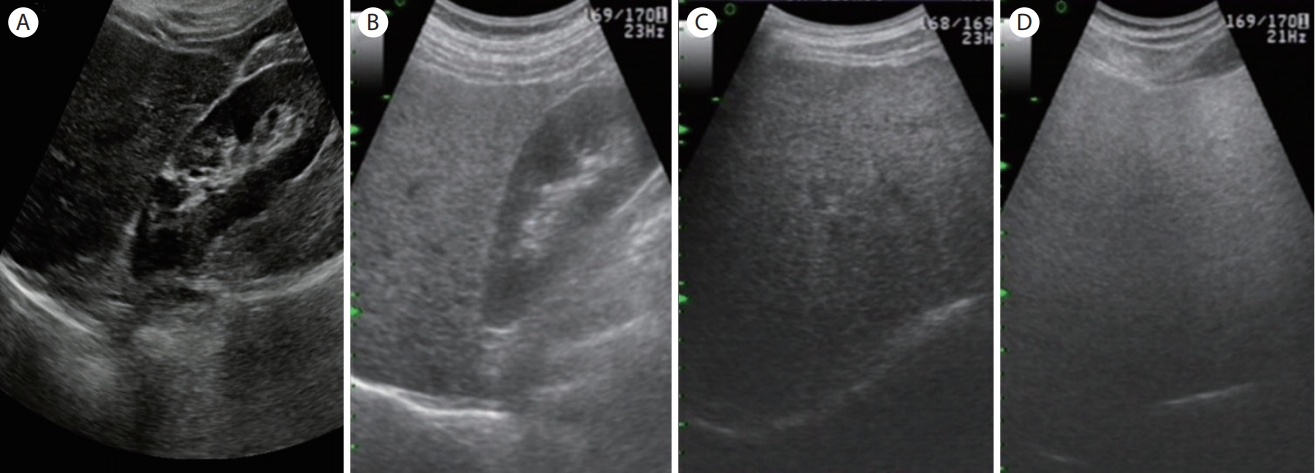
Figure 18.
Measurement of liver size. (A) Left lobe: cranio-caudal length (a to b) and antero-posterior length (a to c). (B) Right lobe: longitudinal length in right longitudinal scan at anterior axillary line or mid-clavicular line (inferior end of the right lobe to the diaphragm parallel to the long axis of the right kidney, a to b). (C) Right lobe: antero-posterior length in right subcostal scan at midclavicular line (a to b). 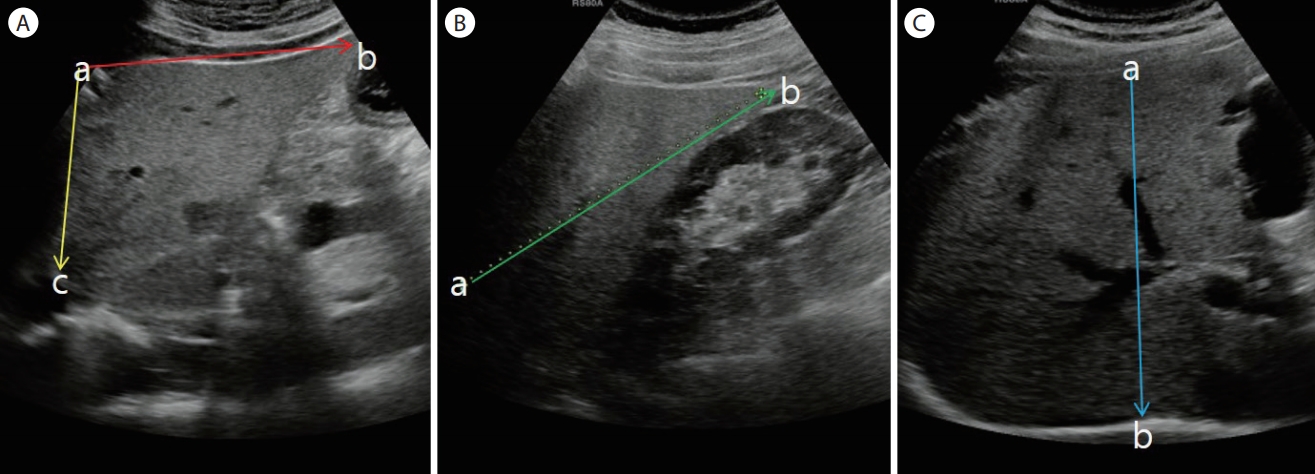
Figure 19.
Characteristics of different lesions. (A) Liver cyst (anechoic, round). (B) Small liver hemangioma (hyperechoic, no mass effect). (C) Liver hemangioma in fatty liver (hypoechoic due to fatty liver). (D) Huge liver hemangioma (mixed echo, no mass effect). (E) Small hepatocellular carcinoma (hypoechoic). (F) Small hemangioma-like hepatocellular carcinoma (hyperechoic with peripheral halo, by Son Jun Hyuk). (G) Advanced hepatocellular carcinoma (mixed echo, mosaicism, peripheral halo). (H) Metastatic liver cancer (cluster sign). 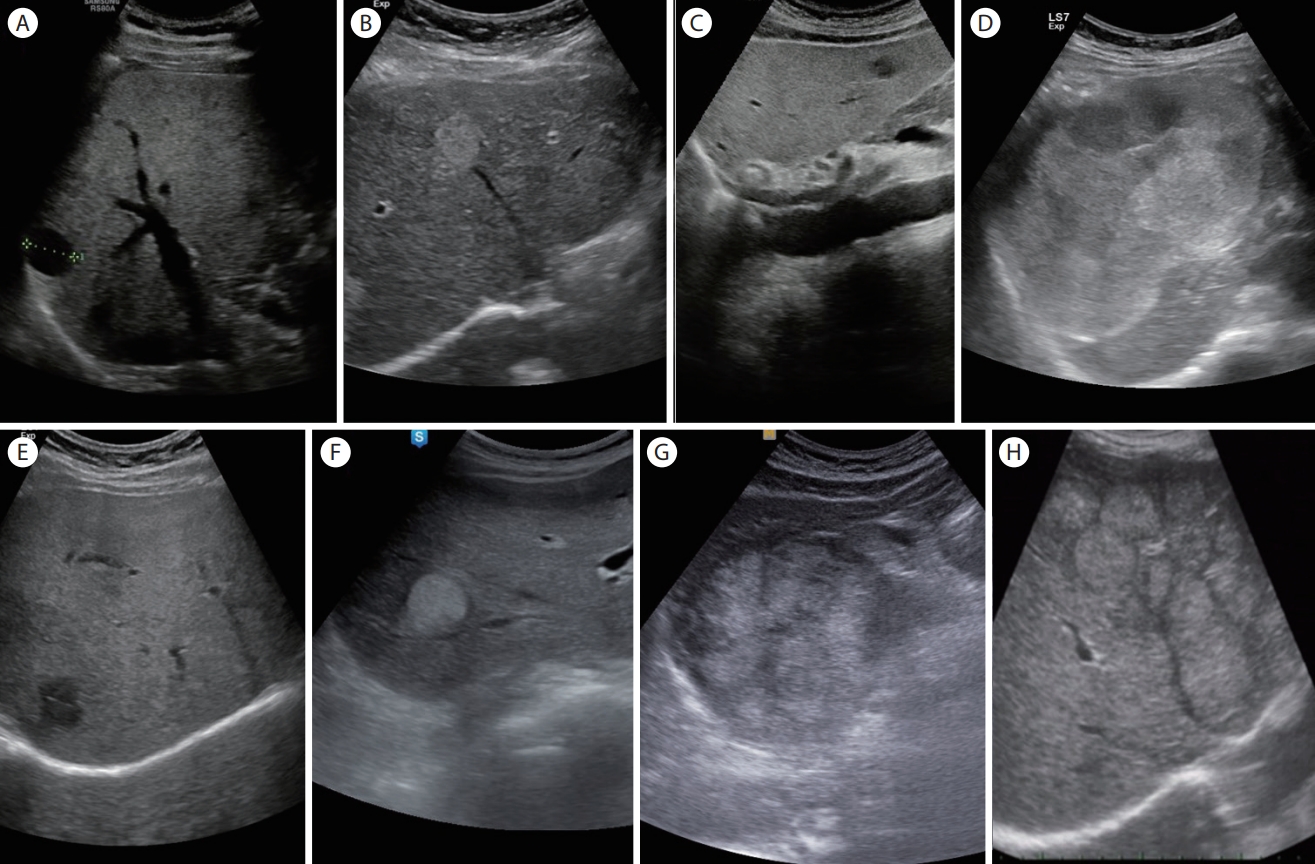
Figure 20.
Detection of portal vein thrombosis and measurement of portal vein. (A) Size of portal vein (>13 mm, portal vein dilatation). (B) Benign portal vein thrombosis. (C) Malignant portal vein thrombosis (increased portal vein size at thrombosis, blood flows in thrombi on Color Doppler, mass lesion near the thrombosis). 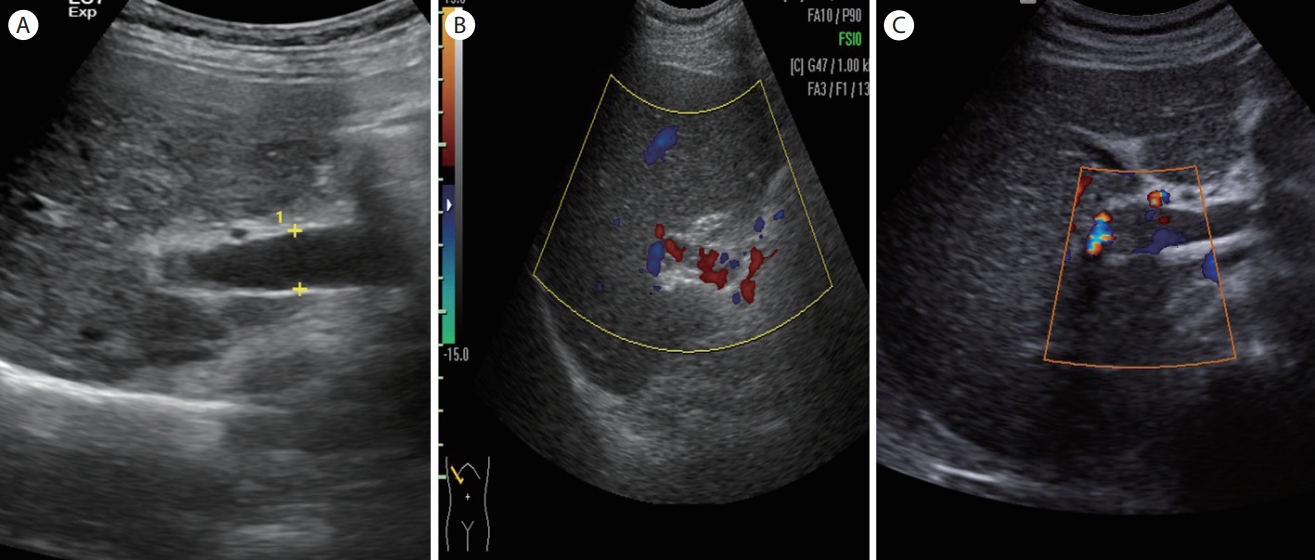
Figure 21.
Basic liver scan according to insurance rule. (A) Longitudinal scan of left lobe of liver (S1-3, ligamentum venosum), (B) transverse scan of left lobe of liver (S1-4, ligamentum venosum, umbilical portion of left portal vein), and (C) hepatic veins on subcostal scan (LHV, MHV, RHV). (D) Transverse or subcostal scan of right lobe of liver (S5-7). (E) Intercostal scan of right lobe of liver including right portal vein (S5, S8, anterior branch of right portal vein). (F) Coronal scan of inferior portion of right lobe of liver and renal cortex. (G) Liver dome, (H) long axis scan of spleen (detail scan). (I) Portal confluence scan, (J) intercostal scan of right lobe of liver including right hepatic vein (S5-8 and RHV). 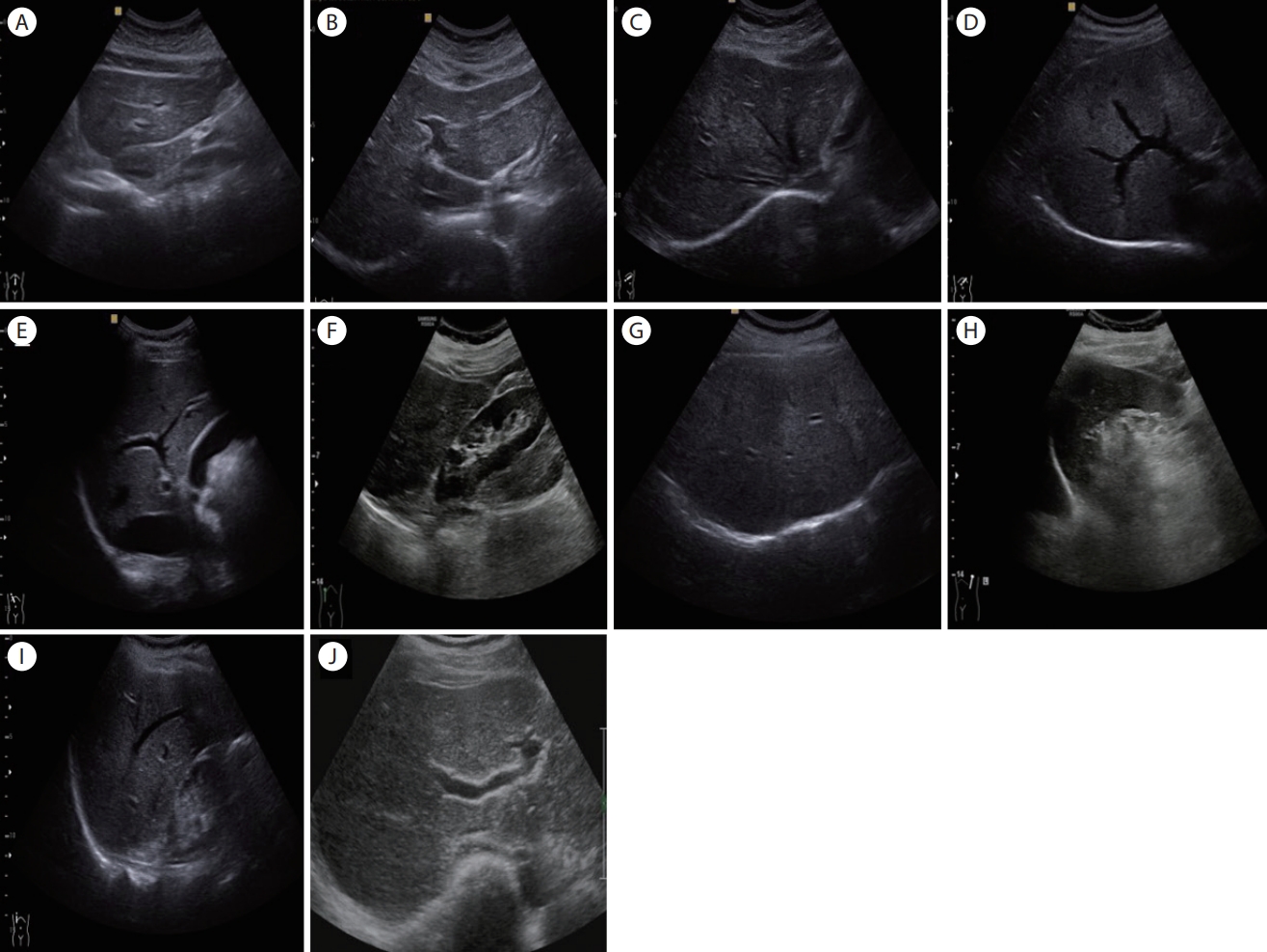
REFERENCES
1. Shim CS. Abdominal ultrasound. 3rd ed. Seoul: Ryo Moon Gak, 2007.
2. Choi BI. Upper abdominal ultrasound diagnosis. 1st ed. Seoul: Ilchokak, 1997.
3. Lee MY, Kim IB. Easy learning to ultrasound wave. 1st ed. Seoul: Bum Moon Education, 2018.
4. Ahuja AJ, Griffith JF, Wong KT, Antonio GE, Chu WC, Ho SS. Diagnostic imaging: ultrasound. 1st ed. Salt Lake City: Amirsys Inc., 2007.
5. Onwuchekwa RC. Radiological anatomy of the liver. Journal of Medicine and Medical Sciences 2016;7:72–78.
6. Maruyama K, Yakuwa T, Kudo T, Mitsuzuka S. Basic abdominal ultrasound. Kim IB, Kim HJ, Translator and Editor. 1st ed. Seoul: Median Book, 2017.
10. Kim YK, Han DK. Liver size measurement method by ultrasonography and reference range based on normal adult physique index. J Radiol Sci Technol 2018;41:13–24.  11. Al-Nakshabandi NA. The role of ultrasonography in portal hypertension. Saudi J Gastroenterol 2006;12:111–117. 
|
|