근골격계 초음파의 활용
Abstract
Musculoskeletal ultrasound is a safe, reliable, and inexpensive alternative to other imaging modalities. Ultrasound is utilized by clinicians both diagnostically and therapeutically. It can be used to assess inflammatory and non-inflammatory conditions of the joints and peri-articular structures. Utilizing musculoskeletal ultrasound for invasive procedures, such as aspiration and injection of joints, bursa, and tendon sheaths, allows for improved precision and increases patient satisfaction.
Keywords: Musculoskeletal ultrasound; Musculoskeletal diseases; Rheumatic diseases
중심 단어: 근골격계 초음파; 근골격계 질환; 류마티스 질환
서 론
정상과 비정상 근골격 조직의 초음파에 대한 설명이 각각 1958년과 1972년부터 시작된 이후로 탐촉자 및 영상을 구현하는 컴퓨터 기술의 발전으로 말미암아 현재는 근골격 질환에 있어 근골격계 초음파는 진단 및 치료에 매우 중요한 도구가 되었다[ 1, 2]. 근골격계 초음파는 방사선 노출 없이 연골과 연부조직, 체액 등을 관찰할 수 있으며, 골 표면을 좀 더 정밀하게 관찰할 수 있다는 점이 자기공명영상과 유사하면서도 이점이 된다. 전산화단층촬영이나 자기공명영상과 비교하여 비교적 비용이 저렴하고 특별한 금기사항이 없으며 여러 관절을 한꺼번에 관찰할 수 있고 조영제를 사용하지 않고 검사할 수 있다는 장점이 있다. 또한 실시간 검사가 가능하여 검사 중 환자와 상호작용을 통하여 자세를 변경해 가며 검사할 수 있다. 탐촉자를 활용하여 직접 눌러서 압통을 확인하는 등 신체 검사를 보완할 수 있으며 주사 치료 시 초음파 유도를 통하여 정확한 시술을 가능하게 한다. 하지만 초음파의 주파수가 골 내로 침투할 수 없기 때문에 골수부종이나 골 내부 병변을 관찰하는 데 한계가 있다. 검사자의 숙련도와 경험에 따라 영상의 질과 해석이 달라질 수 있어 적절한 교육과 수련이 필요하다[ 3, 4]. 본 종설에서는 이러한 장단점을 지닌 근골격계 초음파의 효과적인 활용에 관하여 논하고자 한다.
본 론
근골격계 초음파의 준비
근골격계 초음파 검사를 시행하기 위해서는 기본적으로 7.5 MHz 이상의 선형 탐촉자가 구비된 초음파 기계가 필요하다. 탐촉자에서 방출된 초음파의 주파수에 따라 투과력과 해상력이 결정되는데, 이 두 인자는 서로 반비례 관계로 주파수가 높을수록 투과력이 감소하여 관찰할 수 있는 조직의 깊이는 감소하나 해상력이 증가하여 세밀한 영상을 얻을 수 있다. 따라서 관찰하고자 하는 부위에 따라 적절한 탐촉자의 선택이 중요하다. 손목, 손가락, 발가락 관절과 같이 표면에 위치한 관절은 10 MHz 이상의 주파수를 사용하며, 고관절처럼 상대적으로 깊게 위치해 있는 관절은 5-10 MHz 정도의 상대적으로 낮은 주파수의 탐촉자를 사용한다. 최근의 선형 탐촉자는 광대역(broadband) 주파수(예: 7-18 MHz)를 사용하므로 한 개의 탐촉자로 모든 활막관절을 관찰할 수 있다. 아울러 초음파의 발생, 영상 형성의 기본 원리, 회색도(grey-scale)와 도플러 초음파 원리 및 초음파 허상(artifact)에 대한 기본적인 지식과 이해가 깊을수록 좋은 영상을 얻는 데 도움이 된다( Table 1) [ 5]. 또한 관찰하고자 하는 근골격계의 해부학 및 초음파 영상해부학에 대한 지식과 이해가 필요하고 이를 바탕으로 초음파 영상에서 가장 잘 보이기 위한 표준 스캔 방법을 습득하여야 한다. 근골격계 초음파의 병변이 의심될 경우 반드시 2부위의 수직면(two perpendicular planes – longitudinal and transverse plane)으로 모두 관찰하여 판단해야 한다.
근골격계 초음파의 주요 구조물과 병변의 초음파 소견
기본 구조물의 초음파 소견
구조물들의 형태에 따라 흑백으로 영상이 표현되며 밝기(echogenicity)와 모양(pattern)을 보고 구조물들과 병변을 이해하게 된다( Table 2) [ 6].
류마티스 질환의 초음파 소견
2005년 Outcome Measures in Rheumatology (OMERACT) Ultrasound (US) Working Group (WG)에서 류마티스 질환의 핵심적인 병변들에 대한 관절 초음파 소견의 정의를 발표하였고 2019년도에 염증성 병변, 구조적 병변으로 나누어 갱신하였다( Table 3) [ 7]. 환자에서 여러 가지 소견이 관찰될 수 있어 초음파 병변을 판독하기 위해서는 문진과 신체 진찰을 통한 환자의 파악이 선행되어야 한다.
근골격계 초음파의 진단적 활용
류마티스관절염
활막염, 힘줄 활막염, 골미란 등의 여부를 관찰하며 회색도모드와 도플러모드를 이용하여 질병 활성도 평가를 한다.
활막삼출(synovial effusion)
관절 내에서 비정상 저에코 또는 피하지방에 비하여 무에코 소견으로 관찰되며, 변위(displacement)나 압축(compression)이 가능하고 도플러 신호가 나타나지 않는다( Fig. 1A, B).
활막비대(synovial hypertrophy)
관절낭 안에 존재하는 비정상적인 저에코 소견으로 관찰되며 변위, 압축되지 않고 도플러 신호가 나타날 수 있다( Fig. 1A, B).
골미란(eorison)
골표면의 불연속성이 2개의 수직면에서 관절 내 및 또는 관절 외에서 관찰된다( Fig. 1A). 2017년 OMERACT US WG와 유럽 류마티스 연맹(European League Against Rhueumatism)이 공동으로 류마티스관절염의 활막염 평가 기준을 반정량화 형태로 제시하여 질병 활성도를 평가, 비교가 가능하다( Table 4) [ 8].
골관절염
골극(osteophyte)
뼈의 가장자리 부분에서 위쪽으로 상승된 뼈의 돌출 부분이 2개의 수직 단면에서 관찰된다( Fig. 1C).
연골 손상(cartilage damage)
무에코 구조물의 손실 및 또는 연골층의 얇아짐이 관찰되거나 적어도 한 부분의 연골 가장자리의 불규칙성 및 또는 날카로움이 관찰된다( Fig. 1D).
강직척추염
부착부염(enthesitis)
골부착부(골 피질로부터 2 mm 이내)에서 저에코 및 또는 두꺼워진 힘줄이나 인대가 관찰되고 활성도가 높을 경우 도플러 신호가 나타난다. 구조적인 손상이 있을 경우 골미란이나 부착부골극(enthesophyte) ( Fig. 1B), 석회화가 관찰된다.
통풍
이중윤곽징후(double contour sign)
관절 연골의 경계에 초음파의 각도와 무관하게 비정상적인 고에코를 나타내는 띠로 표현되며, 이는 규칙적일 수도 비규칙적일 수도 있고, 연속적일 수도 간헐적일 수도 있다.
통풍결절(tophus)
명확하게 경계가 지어진 고에코 및/또는 저에코가 섞여 있는 불균질한 에코를 띄는 응집체이며, 무에코의 테두리로 둘러싸여 있다( Fig. 1E).
집합체(aggregate)
비균질의 고에코성 병소로 후방음향이 동반되기도 한다. 최근 OMERACT group에서 집합체를 평가할 때 관찰자 간의 일치도가 낮아 평가 시스템 개발 과정에서 새로운 정의를 제시하였다. 통풍 결절의 정의를 충족시키기에는 매우 작고 밝은 고에코성 병소로 입사각이 변경되더라도 높은 반사도를 유지하는 점이 특징이다[ 9].
칼슘피로인산결정침착질환
탐촉자로 동적 검사 과정에서 후방음영 없이 움직이거나 고정되어 관찰 가능한 다양한 크기와 모양의 고에코 침전물이 연골( Fig. 1F), 인대, 활액 등에서 관찰된다.
근골격계 초음파의 치료적 활용
손가락, 발가락, 손목 등과 같은 작은 관절을 비롯하여 모든 관절의 천자 및 스테로이드 주사에서 초음파 유도하에 시술이 가능하다. 또한 점액낭염, 농양, 혈종, 결절종, 베이커씨 낭종 등과 같은 병변의 천자, 방아쇠 손가락(trigger finger), 수근관증후군의 스테로이드 주사 및 석회성 힘줄염의 흡인 초음파 유도하의 시술을 할 수 있다. 초음파 유도하의 시술은 많은 장점이 있다. 바늘의 삽입, 진입, 천자, 주사의 전 과정 동안 바늘의 위치를 실시간으로 확인하며 시술을 할 수 있다. 바늘 위치의 정확성으로 맹목 주사(blind injection)가 어려운 연부조직을 포함한 모든 시술 과정에서 초음파 유도를 이용한 시술은 치료 결과를 효율적으로 향상시킨다[ 10, 11].
결 론
근골격계 초음파는 근골격 질환의 진단, 치료, 시술에서 많은 임상적 활용이 가능하고 또한 도플러 초음파를 통해 얻을 수 있는 관류에 대한 정보로 염증성 정도를 판단하여 질병 활성도를 측정하는 데 유용하다. 관절 천자 및 주사에 있어 초음파 유도하의 시행은 정확성을 통해 진단 및 치료의 효율을 높인다는 의미에서 환자 진료에 매우 유용하다고 할 수 있다. 하지만 이에 앞서 철저한 문진과 신체진찰이 선행되어야 근골격계 초음파도 그 활용도가 증대될 수 있다.
Figure 1.
Musculoskeletal ultrasound of rheumatic diseases. (A) Erosion and synovial hypertrophy with Doppler activity of elbow. Bone erosion (arrow) and hypoechoic synovial hypertrophy (arrow) were observed on the medial side of the elbow, and a Doppler signal indicating disease activity was observed around the synovial hypertrophy in Doppler mode. (B) Synovial effusion, synovial hypertrophy and enthesophyte of the knee. Enthesophyte (arrow) was observed at the quadriceps femoris ligament enthesis site, and hypoechoic synovial effusion (arrow) and synovial hypertrophy (arrow) were observed. (C) Osteophytes of the Knee. A decrease in joint space on the medial side of the knee and osteophytes (arrows) of the femur and tibia were observed. (D) Cartilage damage of the knee. Decrease (arrow) and irregularity of the knee joint cartilage layer were observed. (E) Tophi of the Knee. Tophi (arrow), which were aggregations of heterogeneous echoes, were observed in the upper part of the patella. (F) Calcium deposits within the cartilage of the knee. Linear hyperechoic deposits (arrow) were observed inside the knee cartilage layer. 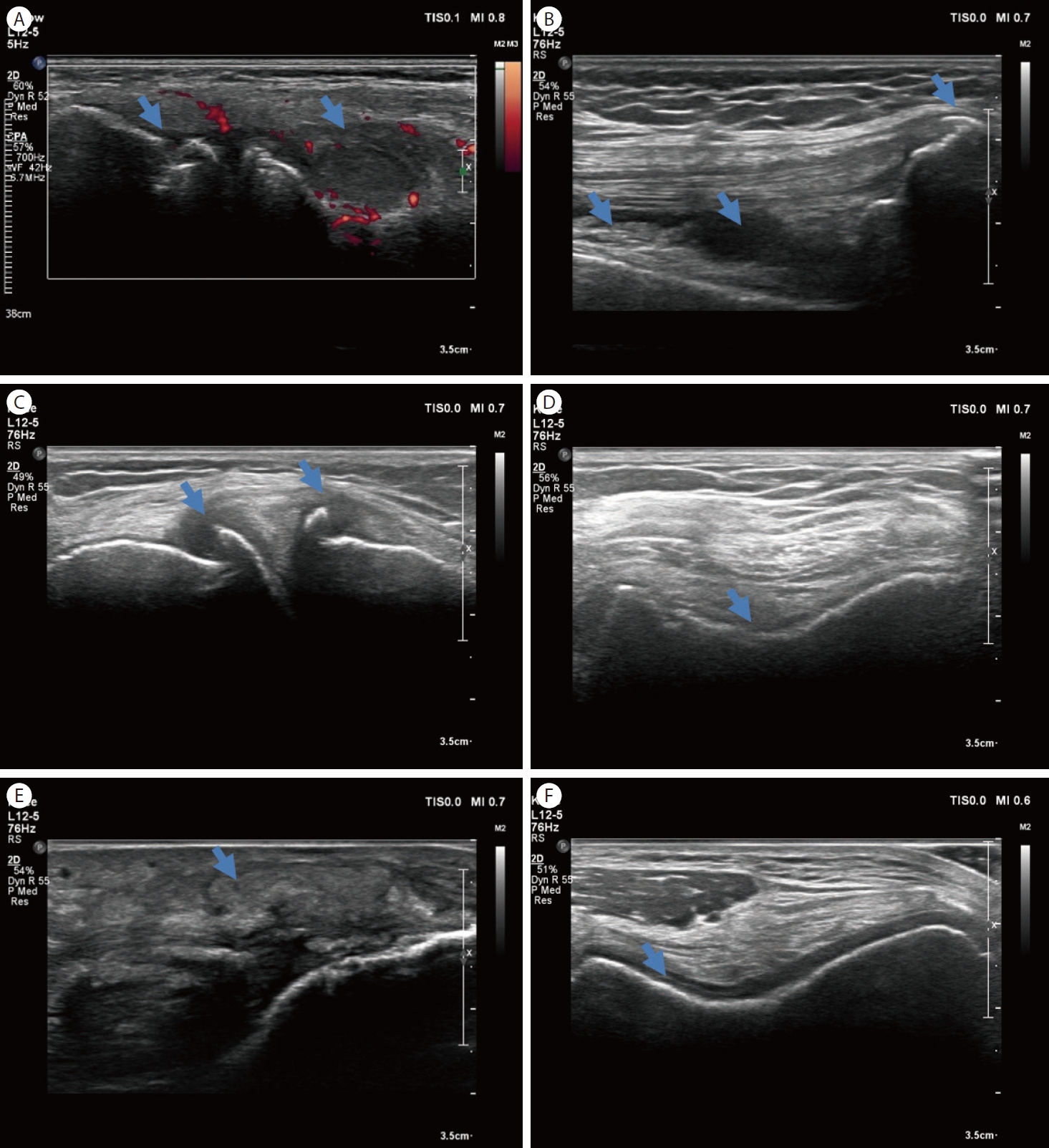
Table 1.
Knowledge and skills for musculoskeletal ultrasound
|
Anatomy/pathology |
|
MUS equipment/physics/artifact |
|
Indication/limitations of MUS |
|
Clinical application/relevance |
|
Machine functions/operation |
|
Image optimization |
|
Dynamic assessment |
|
Color Doppler/power Doppler |
|
Patient/probe position |
|
Planes and system of examination |
Table 2.
Echogenic properties of musculoskeletal structures
|
Structure |
Echogenic property |
|
Bone surface |
Bright and hyperechoic with posterior acoustic shadowing |
|
Hyaline cartilage |
Anechoic and black |
|
Fibrocartilage |
Hyperechoic |
|
Ligament |
Fibrillar pattern like that of tendons, but fibers may run in different directions |
|
Tendon |
Fine internal fibrillar pattern, hyperechoic if localized perpendicular to the probe |
|
Joint capsule |
Hyperechoic |
|
Synovium |
Hypoechoic |
|
Synovial fluid |
Anechoic |
|
Bursa |
Hypoechoic or anechoic depending on the structures in the bursa |
|
Nerve |
Similar but more dotted, less echogenic and less fibrillar than tendons |
|
Muscle |
Hypoehoic and fine intramuscular hyperechoic lines represent the epi-and perimysium |
Table 3.
Definition of the elementary lesions composing the ultrasound pathologies
|
Pathology |
Definition |
|
Synovitis |
Synovial hypertrophy is defined as the presence of abnormal hypoechoic synovial tissue within the capsule that is not displaceable and poorly compressible and that may exhibit Doppler signals. |
|
Enthesitis |
Hypoechoic increased thickness of anatomical enthesis (i.e., tendon insertion < 2 mm from the bony surface) that exhibits Doppler signal. |
|
Calcifications/enthesophytes at enthesis, erosions at enthesis. |
|
Tenosynovitis |
Tenosynovial hypertrophy is defined as the presence of abnormal hypoechoic (relative to tendon fibers) tissue within the synovial sheath that is not displaceable and poorly compressible, and seen in 2 perpendicular planes; it may exhibit Doppler signals. |
|
Tendon damage |
Internal and/or peripheral focal tendon defect (i.e., absence of fibers) in the region enclosed by tendon sheath, seen in 2 perpendicular planes; the grade of tendon damage should be assessed in both planes. |
|
Erosion |
Intra- and/or extraarticular discontinuity of bone surface (visible in 2 perpendicular planes). |
|
OA osteophyte |
Step-up bony prominence at the bony margin that is visible in 2 perpendicular planes. |
|
OA hyaline cartilage damage |
Loss of anechoic structure and/or thinning of cartilage layer, and irregularities and/or sharpness of at least 1 cartilage margin. |
|
Gout DC sign |
Abnormal hyperechoic band over the superficial margin of the articular hyaline cartilage, independent of the angle of insonation which may be either irregular or regular, continuous or intermittent and can be distinguished from the cartilage interface sign. |
|
Gout tophus |
Circumscribed, inhomogeneous, hyperechoic and/or hypoechoic aggregation (which may or may not generate posterior acoustic shadow), which may be surrounded by a small anechoic rim. |
|
Gout aggregates |
Heterogeneous hyperechoic foci that maintain their high degree of reflectivity, even when the gain setting is minimized or the insonation angle is changed and which occasionally may generate posterior acoustic shadow. |
|
CPPD fibrocartilage |
Hyperechoic deposits of variable shape, localized within the fibrocartilage structure, that remain fixed or move along with the fibrocartilage during dynamic assessment. |
|
CPPD hyaline cartilage |
Hyperechoic deposits of variable size and shape, without posterior shadowing, localized within the hyaline cartilage, that remain fixed and move along with the hyaline cartilage during dynamic assessment. |
|
CPPD tendon |
Hyperechoic, linear structure(s) generally without posterior shadowing, localized within the tendon and remaining fixed and moving along with the tendon during dynamic assessment. |
|
CPPD synovial fluid |
Hyperechoic deposits of variable size, localized within the synovial fluid, without posterior shadowing, and mobile along with joint movement and probe pressure. |
Table 4.
EULAR-OMERACT scoring system
|
Grade |
Definition |
|
Grey-scale |
|
|
|
Grade 0 (normal) |
No synovial hypertrophy independently of the presence of effusion |
|
Grade 1 (minimal) |
Synovial hypertrophy with or without effusion up to the level of the horizontal line connecting bone surfaces metacarpal head and proximal phalanx |
|
Grade 2 (moderate) |
Synovial hypertrophy with or without effusion extending beyond joint line but with upper surface convex (curved downwards) or hypertrophy extending beyond the joint line but with upper surface flat |
|
Grade 3 (severe) |
Synovial hypertrophy with or without effusion extending beyond joint line but with upper surface flat or concave (curved upwards) |
|
Power Doppler |
|
|
Grade 0 (normal) |
No Doppler activity |
|
Grade 1 (minimal) |
Up to three single Doppler spots or up to one confluent spot and two single spots or up to two confluent spots |
|
Grade 2 (moderate) |
Greater than grade 1 but < 50% Doppler signals in the total grey-scale background |
|
Grade 3 (severe) |
Greater than grade 2 (> 50% of the background grey-scale) |
|
Combined score |
|
|
Grade 0 (normal) |
No synovial hypertrophy and no Doppler signal |
|
Grade 1 (minimal) |
Grade 1 synovial hypertrophy and ≤ grade 1 Doppler signal |
|
Grade 2 (moderate) |
Grade 2 synovial hypertrophy and ≤ grade 1 Doppler signal or grade 1 synovial hypertrophy and grade 2 Doppler signal |
|
Grade 3 (severe) |
Grade 3 synovial hypertrophy and ≤ grade 3 Doppler signal or grade 1 or 2 synovial hypertrophy and grade 3 Doppler signal |
REFERENCES
1. Dussik KT, Fritch DJ, Kyriazidou M, Sear RS. Measurements of articular tissues with ultrasound. Am J Phys Med 1958;37:160–165.   2. McDonald DG, Leopold GR. Ultrasound B-scanning in the differentiation of Baker’s cyst and thrombophlebitis. Br J Radiol 1972;45:729–732. 3. Guermazi A, Taouli B, Lynch JA, Peterfy CG. Imaging of bone erosion in rheumatoid arthritis. Semin Musculoskelet Radiol 2004;8:269–285. 4. Kang TY. Ultrasonographic findings in rheumatoid arthritis. Korean J Med 2015;89:609–615.  5. Brown AK, O'connor PJ, Roberts TE, Wakefield RJ, Karim Z, Emery P. Recommendations for musculoskeletal ultrasonography by rheumatologists: setting global standards for best practice by expert consensus. Arthritis Rheum 2005;53:83–92. 6. Kang TY. Musculoskeletal ultrasound in rheumatoloty. Korean J Med 2010;78:687–696.
7. Bruyn GA, Iagnocco A, Naredo E, et al. OMERACT definitions for ultrasonographic pathologies and elementary lesions of rheumatic disorders 15 years on. J Rheumatol 2019;46:1388–1393. 9. Christiansen SN, Filippou G, Scirè CA, et al. Consensus-based semi-quantitative ultrasound scoring system for gout lesions: results of an OMERACT Delphi process and web-reliability exercise. Semin Arthritis Rheum 2021;51:644–649. 10. Epis O, Iagnocco A, Meenagh G, et al. Ultrasound imaging for the rheumatologist. XVI. Ultrasound-guided procedures. Clin Exp Rheumatol 2008;26:515–518. 11. del Cura JL. Ultrasound-guided therapeutic procedures in the musculoskeletal system. Curr Probl Diagn Radiol 2008;37:203–218.
|
|