만성 B형간염 환자에서 Shear Wave Elastography의 임상적 의의
Abstract
Chronic liver disease is one of the leading causes of significant morbidity and mortality. Accurate evaluation of liver fibrosis is important because management and prognosis depend on the degree of liver fibrosis. Liver biopsy has been gold standard for evaluating the degree of liver fibrosis in patients with chronic liver diseases. However, because it is an invasive procedure and can cause serious complication, several serological and radiological noninvasive surrogates have been developed. Of these, excellent diagnostic accuracy and reproducibility of shear wave elastography (SWE) in patients with chronic liver diseases have been reported in recent studies. Furthermore, it has been also known that SWE can monitor disease progression or predict the risk of developing liver cirrhosis and hepatocellular carcinoma. In this review, we discussed the clinical implications of SWE in patients with chronic hepatitis B.
Keywords: Elastography; Liver fibrosis; Hepatitis B, Chronic; Liver cirrhosis; Carcinoma, Heptocellular
중심 단어: 간탄력도검사; 간섬유화; 만성 B형간염; 간경변증; 간세포암
서 론
전 세계적으로 만성 간질환은 질병과 사망의 주요 원인 중 하나이다. 간세포 염증 및 괴사가 지속되면 만성 간질환에서 간섬유화가 발생하고, 더욱 진행되면 간경변증이나 간세포암(이하 간암)으로 발전 할 수 있다. 따라서 만성 간질환 환자에서 간섬유화 정도를 평가하는 것은 치료 방침의 결정이나 예후 판정에 매우 중요하다[ 1]. 간조직생검은 간섬유화를 직접 확인하는 것으로 최종적인 진단방법으로 사용되었으나, 침습적인 검사이기 때문에 흔하지는 않지만 검사와 관련된 합병증이 발생할 수 있다. 주요 합병증으로, 출혈, 천공, 감염 등이 있으며, 매우 드물긴 하지만 사망에 이르는 경우도 있다[ 2, 3]. 이에 따라 혈청학적으로 또는 물리적인 방법을 이용하여 비침습적으로 간섬유화를 평가하는 방법들이 개발되어 왔다[ 4]. 이 중에서 특히 shear wave elastography (SWE)는 B-mode 영상에서 간실질의 이상 유무를 확인함과 동시에 실시간으로 간탄력도를 검사할 수 있다는 장점이 있으며, 최근 연구 결과에서는 현재까지 널리 사용되고 있는 transient elastography (TE)와 비교하였을 경우 비슷하거나 우월한 간섬유화 예측력을 보인다는 연구 결과들이 보고되고 있다[ 5- 8]. 본 종설에서는 현재까지 보고된 연구 결과들을 토대로 만성 B형간염에서 SWE를 이용한 간탄력도검사에 대하여 살펴보려 한다.
본 론
측정 방법과 적합성 및 재현성
SWE를 이용한 간탄력도검사는 환자가 오른팔을 머리 뒤로 들어올리고 누운 상태에서 4, 5초간 숨을 참은 채로 우늑간스캔을 통하여 이루어진다. 사다리꼴 컬러박스를 간실질에 위치시켜 신호를 얻으며 컬러박스의 엘라스토그램 신호가 안정기에 도달한 것으로 판단되면 영상을 멈춘다. 컬러박스 안에 큰 혈관이나 결절이 없어 엘라스토그램 신호가 균질한 곳에 region of interest (ROI; Q-box, Fig. 1)를 위치시켜 간탄력도를 측정한다. SWE를 이용한 간탄력도검사는 복수의 영향을 받지 않고 큰 혈관을 피하여 측정할 수 있으며 숙련된 검사자의 경우 검사의 신뢰성을 직접 판단할 수 있다는 장점이 있다[ 9]. SWE를 이용한 간탄력도를 측정 시에 몇 번 측정하는 것이 적합한지에 대해서는 아직 정해진 바가 없지만 이전의 연구들에서 3-5회의 측정을 권고하고 있으며[ 10- 12], 재현성도 비교적 좋은 것으로 알려져 있다[ 13, 14].
정상 수치
SWE의 정상 간탄력도 수치에 대하여 연구들이 진행되었으며 일반적으로 정상 간탄력도의 평균 수치는 4.1-5.1 kPa로 알려져 있다( Table 1). 이러한 결과는 의미 있는 간섬유화(≥ F2)의 cutoff 값인 7-9 kPa보다 낮아 정상인들 중에서 간질환 환자를 구별해 낼 수 있다. SWE를 이용한 간탄력도 수치는 남성에서 더 높은 경향을 보였으며 나이, 체질량지수, 지방간과는 연관이 없었다. 음식물 섭취 후에는 간탄력도 수치가 증가할 수 있어 최소 4시간 이상 금식 후 검사하는 것을 권고하며 그 외에 카페인, 흡연, 운동도 결과에 영향을 줄 수 있다[ 15- 18].
만성 B형간염 환자에서 간섬유화의 예측
SWE를 이용하여 간섬유화 정도를 평가하기 위하여 만성 B형간염 환자에서 가장 많은 연구가 이루어졌으며, 간섬유화 단계와 양의 상관관계를 보였다( Table 2). 의미 있는 간섬유화(≥ F2)에 대하여 area under the receiver operating characteristic curve는 0.880에서 0.970으로, 그에 따른 cutoff 값은 7.1에서 7.6 kPa로 보고되었다[ 5- 8]. 또한 모든 연구에서 SWE는 TE보다 섬유화 단계 예측에 우수한 진단 성능을 보였다[ 5- 8].
간세포암 발생 위험도 예측
원인에 상관 없이 간경변증이 간암 발생의 가장 중요한 위험인자라는 것은 명백하다. B형간염에 의한 간경변증 환자에서는 연간 간암 발생률이 3-8%, C형간염에 의한 간경변증 환자에서는 연간 간암 발생률이 1-7%로 보고된다[ 19]. 간경변증의 진단은 초음파검사와 생화학검사를 바탕으로 임상적으로 이루어지지만 초음파검사의 경우 검사자에 따른 해석의 편차가 컸기 때문에 간경변증은 어느 정도 형태학적인 변화를 보이는 단계까지 진행이 되었을 때 진단이 가능하였다. 하지만 SWE를 이용한 간탄력도검사는 대상성 간경변증을 조기 진단할 수 있다는 장점이 있다. 뿐만 아니라 간경변증을 조기에 진단함으로써 간암 발생의 위험을 예측할 수 있다. Hamada 등[ 20]의 연구에서 C형간염 환자에서 SWE를 이용한 간탄력도 측정 결과가 높은 경우에 간암 발생이 유의하게 증가하였다( Table 3). Jeong 등[ 21]의 연구에서 만성 B형간염 환자에서도 SWE를 이용한 간탄력도 측정 결과가 높은 경우에 간암 발생이 유의하게 증가하였다( Table 3 and Fig. 2). 이러한 결과는 TE를 이용하여 간섬유화의 정도와 간암 발생과의 관련성을 연구하였던 결과들과 일치한다[ 22, 23].
결 론
만성 간질환 관리에 있어서 비침습적 방법으로 간섬유화 정도를 평가하는 것은 매우 중요하다. SWE와 같은 간탄력도검사를 통하여 정상인들 중에서 간질환이 의심되는 환자들을 구별해 낼 수 있고, 만성 간질환을 가진 환자 중에서 의미 있는 간섬유화, 간경변증을 가진 환자들을 구별할 수 있고, 간암 발생의 위험을 예측할 수 있다. 최근 연구 결과에 따르면 SWE는 TE보다 간섬유화 예측에 비슷하거나 우월한 정확성을 보였고, TE와 달리 복수가 있는 환자에서도 시행할 수 있다는 장점이 있다. 하지만 아직까지 SWE를 이용한 간탄력도검사에 대한 연구가 많지 않아 대규모의 전향적 연구가 더 많이 필요할 것으로 생각된다.
Figure 1.
Shear wave elastography images. Color box (arrow) and Q-box (curved arrow). 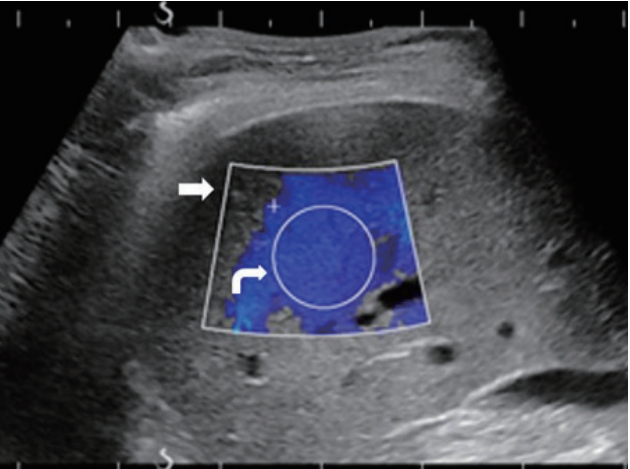
Figure 2.
The cumulative incidence of hepatocellular carcinoma according to liver stiffness values by SWE. HCC, hepatocellular carcinoma; SWE, shear wave elastography. 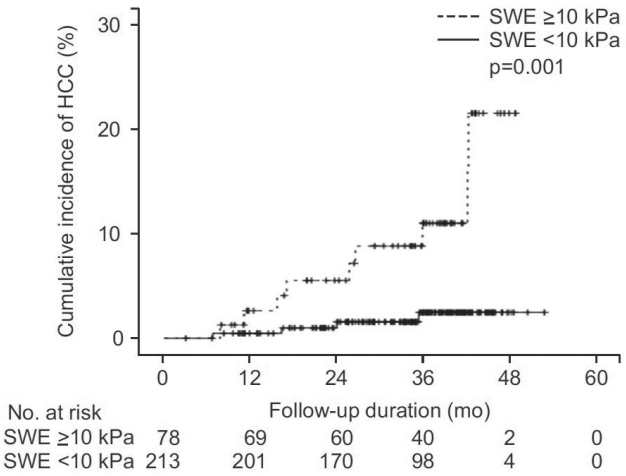
Table 1.
Normal liver stiffness values by SWE
|
Suh et al. [13] |
Ma et al. [24] |
Huang et al. [25] |
Mulabecirovic et al. [26]
|
Serra et al. [27] |
Bende et al. [28] |
|
GE |
Samsung |
|
Number of subjects |
196 |
84 |
502 |
100 |
54 |
79 |
|
Population |
Liver donors |
Healthy volunteers |
Healthy volunteers |
Healthy volunteers |
Healthy volunteers |
Healthy volunteers |
|
Liver stiffness (kPa) |
4.4 (mean) |
4.62 (mean) |
5.1 (mean) |
4.5 (mean) |
4.1 (mean) |
4.65 (mean) |
5.1 (mean) |
|
95th percentile (kPa) |
- |
- |
5.02-5.19 |
4.37-4.67 |
3.91-4.23 |
- |
- |
|
Body mass index (kg/m2) |
22.8 (mean) |
- |
21.3 (mean) |
- |
- |
- |
- |
|
Effects on SWE |
|
|
|
|
|
|
|
|
Age |
- |
No |
No |
No |
No |
No |
Increased with age |
|
Gender |
|
No |
M > F |
M > F |
No |
M > F |
M > F |
|
High body mass index |
No |
- |
No |
- |
- |
No |
No |
|
Fatty liver |
No |
No |
- |
- |
- |
- |
- |
Table 2.
Diagnostic performance of shear wave elastography for significant fibrosis (F ≥ 2), advanced fibrosis (F ≥ 3), and cirrhosis (F4) in patients with chronic hepatitis B
|
Herrmann et al. [8]
|
Zeng et al. [6]
|
Zhuang et al. [7]
|
Leung et al. [5]
|
|
F ≥ 2 |
F ≥ 3 |
F = 4 |
F ≥ 2 |
F ≥ 3 |
F = 4 |
F ≥ 2 |
F ≥ 3 |
F = 4 |
F ≥ 2 |
F ≥ 3 |
F = 4 |
|
379 |
|
|
257 |
|
|
304 |
|
|
226 |
|
|
|
Patients (%) |
52 |
29.8 |
13 |
46.3 |
24.9 |
13.2 |
86.8 |
70.4 |
54.9 |
60.2 |
35.4 |
15.5 |
|
Cutoff (kPa) |
7.1 |
8.1 |
11.5 |
7.1 |
8.3 |
11.3 |
7.6 |
9.2 |
10.4 |
7.1 |
7.9 |
10.1 |
|
Sensitivity (%) |
87.6 |
94.9 |
79.9 |
88.89 |
89.66 |
93.55 |
92 |
91.6 |
94.6 |
84.7 |
89.8 |
97.4 |
|
Specificity (%) |
73.6 |
73.1 |
93.9 |
76.38 |
76.84 |
87.25 |
90 |
96.7 |
94.9 |
92.1 |
90.3 |
93 |
|
PPV (%) |
- |
- |
- |
76.2 |
55.9 |
52.7 |
98.4 |
98.5 |
95.7 |
85.3 |
71.8 |
60.1 |
|
NPV (%) |
- |
- |
- |
89 |
95.8 |
98.9 |
64.3 |
82.9 |
93.5 |
91.7 |
97 |
99.6 |
|
AUROC |
0.906 |
0.931 |
0.955 |
0.882 |
0.917 |
0.926 |
0.97 |
0.96 |
0.98 |
0.88 |
0.93 |
0.98 |
Table 3.
Predictive performance of shear wave elastography to predict the risk of developing hepatocellular carcinoma in patients with chronic liver diseases
|
Region |
Patients |
Etiology |
Follow-up (months) |
HCC development |
AUROC |
Cutoff (kPa) |
HR |
p value |
|
Hamada et al. [20] |
Asia |
196 |
HCV |
26 |
8 |
0.933 |
11 |
28.71 |
0.006 |
|
Jeong et al. [21] |
Asia |
291 |
HBV |
35.8 |
13 |
0.783 |
10 |
5.97 |
0.003 |
REFERENCES
1. Castera L. Invasive and non-invasive methods for the assessment of fibrosis and disease progression in chronic liver disease. Best Pract Res Clin Gastroenterol 2011;25:291–303.   2. Dienstag JL. The role of liver biopsy in chronic hepatitis C. Hepatology 2002;36:S152–S160. 3. Bravo AA, Sheth SG, Chopra S. Liver biopsy. N Engl J Med 2001;344:495–500. 4. Lupsor-Platon M, Badea R, Gersak M, et al. Assessment of liver disease using 2D shear wave elastography. J Gastrointestin Liver Dis 2016;25:525–532. 5. Leung VY, Shen J, Wong VW, et al. Quantitative elastography of liver fibrosis and spleen stiffness in chronic hepatitis B carriers: comparison of shear wave elastography and transient elastography with liver biopsy correlation. Radiology 2013;269:910–918. 6. Zeng J, Zheng J, Huang Z, et al. Comparison of 2-D shear wave elastography and transient elastography for assessing liver fibrosis in chronic hepatitis B. Ultrasound Med Biol 2017;43:1563–1570. 7. Zhuang Y, Ding H, Zhang Y, Sun H, Xu C, Wang W. Two-dimensional shear-wave elastography oerformance in the noninvasive evaluation of liver fibrosis in patients with chronic hepatitis B: comparison with serum fibrosis indexes. Radiology 2017;283:873–882. 8. Herrmann E, de Lédinghen V, Cassinotto C, et al. Assessment of biopsy proven liver fibrosis by tow-demensional shear wave elastography: an individual patient data-based meta-analysis. Hepatology 2018;67:260–272. 10. Sporea I, Grădinaru-Taşcău O, Bota S, et al. How many measurements are needed for liver stiffness assessment by 2D-shear wave elastography (2D-SWE) and which value should be used: the mean or median? Med Ultrason 2013;15:268–272. 11. Yoon JH, Lee JM, Han JK, Choi BI. Shear wave elastography for liver stiffness measurement in clinical sonographic examinations: evaluation of intraobserver reproducibility, technical failure, and unreliable stiffness measurements. J Ultrasound Med 2014;33:437–447. 12. Choi SH, Jeong WK, Kim Y, et al. How many times should we repeat measuring liver stiffness using shear wave elastography?: 5-repetition versus 10-repetition protocols. Ultrasonics 2016;72:158–164. 13. Suh CH, Kim SY, Kim KW, et al. Determination of normal hepatic elasticity by using real-time shear-wave elastography. Radiology 2014;271:895–900. 14. Ferraioli G, Tinelli C, Zicchetti M, et al. Reproducibility of real-time shear wave elastography in the evaluation of liver elasticity. Eur J Radiol 2012;81:3102–3106. 15. Arena U, Lupsor Platon M, Stasi C, et al. Liver stiffness is influenced by a standardized meal in patients with chronic hepatitis C virus at different stages of fibrotic evolution. Hepatology 2013;58:65–72. 16. Lemoine M, Shimakawa Y, Njie R, et al. Food intake increases liver stiffness measurements and hampers reliable values in patients with chronic hepatitis B and healthy control: the PROLIFICA experience in The Gambia. Aliment Pharmacol Ther 2014;39:188–196. 18. Gersak MM, Sorantin E, Windhaber J, Dudea SM, Riccabona M. The influence of acute physical effort on liver stiffness estimation using virtual touch qauntification (VTG). Preliminary results. Med Ultrason 2016;18:151–156. 19. EL-Serag HB, Rudlolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology 2007;132:2557–2576. 22. Kim MN, Kim SU, Kim BK, et al. Increased risk of hepatocellular carcinoma in chronic hepatitis B patients with transient elastography-defined subclinical cirrhosis. Hepatology 2015;61:1851–1859. 23. Wong GL, Chan HL, Wong CK, et al. Liver stiffness-based optimization of hepatocellular carcinoma risk score in patients with chronic hepatitis B. J Hepatol 2014;60:339–345. 24. Ma JJ, Ding H, Mao F, Sun HC, Xu C, Wang WP. Assessment of liver fibrosis with elastography point quantification technique in chronic hepatitis B virus patients: a comparison with liver pathological results. J Gastroenterol Hepatol 2014;29:814–819. 25. Huang Z, Zheng J, Zeng J, Wang X, Wu T, Zheng R. Normal liver stiffness in healthy adults assessed by real-time shear wave elastography and factors that influence this method. Ultrasound Med Biol 2014;40:2549–2555. 28. Bende F, Mulabecirovic A, Sporea I, et al. Assessing liver stiffness by 2-D shear wave elastography in a healthy cohort. Ultrasound Med Biol 2018;44:332–341.
|
|