성인에서 갑상선 결절로 쉽게 오인되는 무증상의 이상와누공
요약
갑상선 초음파상 결절이 의심되어 전원된 증례이다. 본원 초음파에서 내부 고음영은 석회화가 아닌 공기에 의한 소견으로 식도조영술로 이상와누공으로 진단하였다. 이상와누공은 드문 질환이지만 경부 초음파에서 공기를 포함한 결절이 관찰될 때는 고려해야 함을 확인하였다.
중심 단어: 이상와; 초음파
Abstract
A pyriform sinus tract/fistula is a rare clinical condition where remnants of the third or fourth pharyngeal pouches extend into the pyriform sinus, forming an internal tract. Common initial presentations of pyriform sinus tract/fistulas are cervical cystic masses in neonates or cervical infections in children but there have been a few reported cases of incidental detection of pyriform sinus tracts in adults. A 62-year-old man was referred from a local clinic for evaluation of a hypoechoic thyroid nodule with calcifications on ultrasonography (US). He had no symptoms of thyroid dysfunction or infection and was euthyroid on laboratory results. Neck US was re-performed in our institution and an air-containing nodule was observed in the posterior aspect of the left thyroid gland. Esophagography was performed to identify this lesion, revealing an obstructed sac structure communicating with the left pyriform sinus. The patient was diagnosed with a pyriform sinus and referred to an otolaryngologist.
Keywords: Pyriform sinus; Ultrasonography
서 론
이상와누공(pyriform sinus tract) 및 이상와루(pyriform sinus fistula)는 드문 기형으로 발생 과정에서 세 번째 혹은 네 번째 인두주머니가 닫히지 않아 발생된다[ 1]. 주로 소아에서 재발되는 경부 감염이나 급성 화농성 갑상선염으로 발견하게 되며, 경부 감염의 재발을 막기 위해 누공절제술(fistulectomy) 혹은 내시경 소작술(endoscopic cauterization)을 통해 농양의 배액을 하게 된다[ 2]. 성인에게서 이상와누공의 보고는 많지 않으나, 소아와 유사하게 경부 감염이나 급성 화농성 갑상선염으로 발견되며, 드물게 갑상선 초음파에서 우연히 발견된 갑상선 결절로 오인되어 보고되기도 한다[ 3, 4]. 저자들은 경부 초음파에서 갑상선 결절로 오인되었던 무증상의 이상와누공의 증례를 문헌고찰과 함께 보고하고자 한다.
증 례
62세 남자가 건강검진을 위해 시행한 갑상선 초음파에서 석회화를 동반한 저에코음영의 갑상선 결절이 의심되어( Fig. 1) 추가적인 평가를 위해 내원하였다. 환자는 이전 갑상선 관련 질환을 진단받은 적은 없었으며, 내원 당시 갑상선 기능이상이나 감염의 징후를 보이지 않았다. 본원에서 시행한 갑상선 기능 검사는 T3 1.01 ng/mL (정상치: 0.61-1.16 ng/mL), free T4 0.76 ng/dL (정상치: 0.80-1.23 ng/dL), 갑상선자극호르몬 1.72 μIU/mL (정상치: 0.41-4.30 μIU/mL)로 정상 범위로 판단되었다. 본원에서 세침흡입 검사 전에 시행한 경부 초음파 검사에서 좌측 갑상선 후방에 13 × 7 mm 경계가 분명한 저에코 결절이 관찰되었고, 결절 내부에 고에코 음영들과 여운허상(ring-down artifact)이 관찰되었다( Fig. 2). 고에코 음영 뒤로 후방음영증강(posterior acoustic enhancement)이 있어 공기를 포함한 병변으로 진단하였다. 병변의 위치와 초음파 소견을 고려하여 식도게실(esophageal diverticulum)의 가능성이 높아 세침흡입 검사는 시행하지 않았다. 확진을 위해 식도조영술을 시행하여 좌측 이상와(pyriform sinus)와 연결된 누공이 확인되어 이상와누공으로 진단하였다( Fig. 3). 이후 본원 이비인후과에서 후두내시경을 통해 좌측 이상와에서 누공으로 연결되는 개구부를 확인하였다( Fig. 4). 특별한 증상 없이 초음파에서 우연히 발견된 이상와누공으로 외래에서 경과 관찰 중이다.
고 찰
이상와누공은 드문 선천성 기형으로 좌측에 호발한다[ 1, 2]. 전체 인두 부위 병변의 약 3-10%로 추정되며 주로 영아나 소아 시기에 발견된다. 영아의 경우 주변 부위를 압박하는 경부 낭종으로 내원하며, 소아는 반복되는 경부 농양 및 급성 화농성 갑상선염으로 내원하는 경우가 많다[ 1]. 식도조영술로 이상와누공 혹은 이상와루를 확진할 수 있으며, 이상와누공 하부에서 시작되는 누공을 시각화할 수 있어 진단에 유용하다[ 5]. 그러나 급성 염증이 동반된 상태에서는 식도조영술에서도 누공이 관찰되지 않을 수 있어 염증이 가라앉고 난 후에 시행하는 것이 좋다[ 6]. 초음파는 이상와누공을 진단하는 데 제한적이지만 2018년 Ahn 등[ 7]이 20명의 이상와누공의 초음파 소견을 분석한 연구에 따르면, 경부 초음파에서 갑상선을 가로지르는 누공, 병변 내 다수의 고에코 병소, 병변 경계의 저에코 테두리 소견 등이 관찰될 때 이상와누공을 의심해볼 수 있다. 특히 갑상선은 아이오딘(iodine)이 풍부하고 두꺼운 섬유질 캡슐로 둘러싸여 있으며 림프관이 잘 발달되어 있어 세균 감염이 드문 장기로[ 3], 갑상선 농양은 갑상선을 통과하는 누공의 존재를 시사한다[ 7]. 병변 내 다수의 고에코 병소 뒤에 공기를 시사하는 초음파 소견이고 석회화의 후방음영그림자(posterior acoustic shadowing)와는 다른 소견이어서 초음파로 공기와 석회화를 구분할 수 있다[ 8]. 경부 초음파에서 이상와누공 외에 갑상선 주변에 공기를 포함하는 병변으로 식도게실과 기관주위공기 낭(paratracheal air cyst)이 있고 이에 대한 감별이 필요하다[ 9, 10]. 본 증례는 경부 초음파에서 갑상선 주변에 고에코 병소를 포함한 결절이 관찰된 경우로 공기와 석회화의 차이를 인지하여 불필요한 세포 검사를 하지 않고 식도조영술 검사를 통해 성인에서 드문 이상와누공을 진단한 증례이다.
Figure 1.
Neck ultrasonography shows a hypoechoic nodule with hyperechogenic foci in the left lobe of the thyroid. 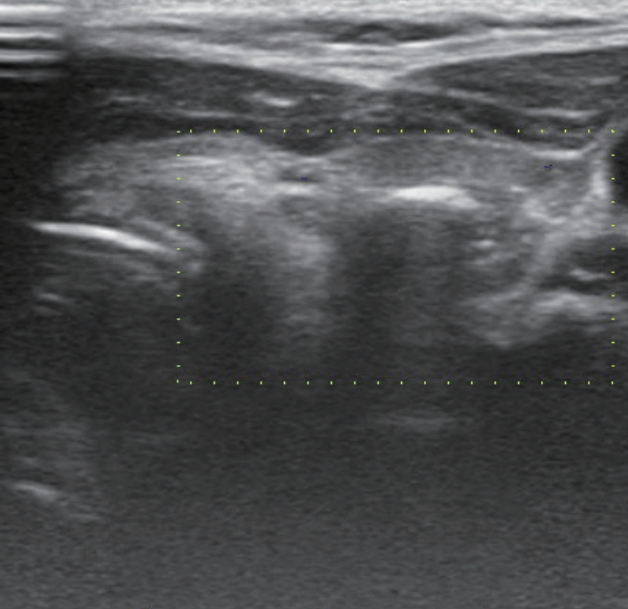
Figure 2.
Neck ultrasonography shows a 13 × 7-mm-sized well-defined hypoechoic nodule with hyperechogenic foci (arrows) and ring-down artifact (arrowheads) in the posterior aspect of the left lobe of the thyroid. (A) Transverse scan. (B) Longitudinal scan. 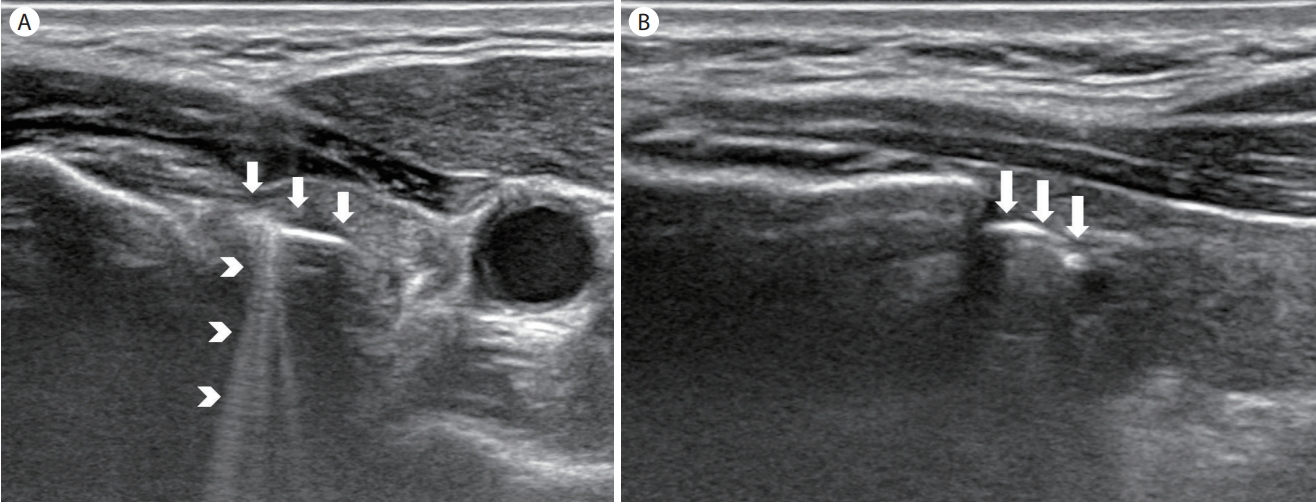
Figure 3.
Esophagography reveals a tract from the left pyriform sinus and accumulation of barium contrast represents the blunt end of the pyriform sinus tract. (A) Frontal view. (B) Lateral view. 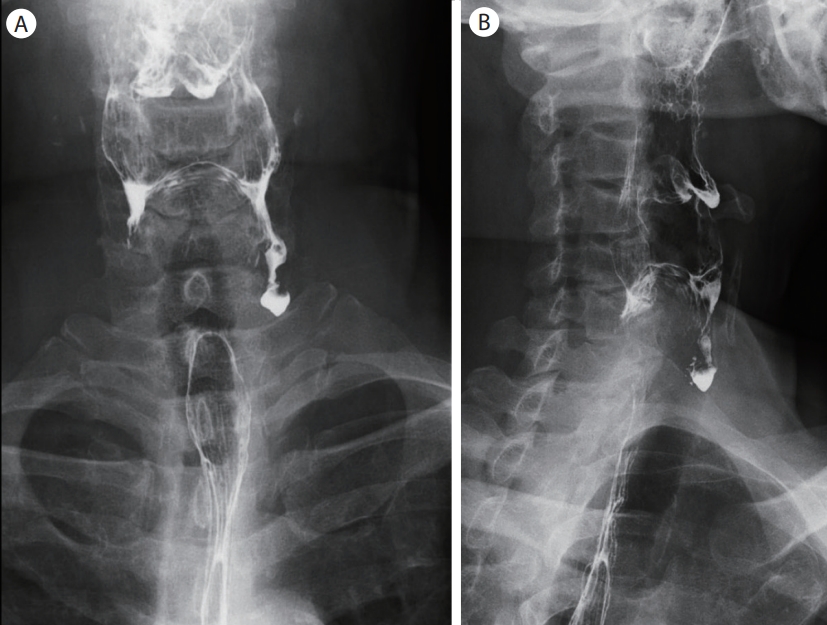
Figure 4.
Laryngoscopy reveals an external opening of the sinus tract in the left pyriform sinus. 
REFERENCES
2. Nicoucar K, Giger R, Pope HG Jr, Jaecklin T, Dulguerov P. Management of congenital fourth branchial arch anomalies: a review and analysis of published cases. J Pediatr Surg 2009;44:1432–1439.   3. Kim SC, Kim JH, Won JK, Chung EJ. Asymptomatic intrathyroidal pyriform sinus fistula mimicking thyroid cancer: a case report and literature review. Medicine (Baltimore) 2018;97:e0488.  6. Hosokawa T, Yamada Y, Takahashi H, et al. Optimal timing of the first barium swallow examination for diagnosis of pyriform sinus fistula. AJR Am J Roentgenol 2018;211:1122–1127. 8. Feldman MK, Katyal S, Blackwood MS. US artifacts. Radiographics 2009;29:1179–1189. 9. Lixin J, Bing H, Zhigang W, Binghui Z. Sonographic diagnosis features of Zenker diverticulum. Eur J Radiol 2011;80:e13–e19.
|
|