하지부종 환자에서 혈관 초음파의 유용성
Abstract
There are many causes of leg swelling or edema. Leg edema due to systemic condition or disease demonstrates chronic, bilateral features, whereas leg edema caused by vascular disease shows more complex clinical features including secondary skin changes and ulcerative lesion, resulting in more complicated clinical outcomes with less frequent early diagnosis and appropriate management. Definite differential diagnosis might not be possible by medical history, clinical features, and physical findings. Vascular ultrasonography (Duplex ultrasound) can be used easily as a bedside diagnostic procedure and is a recommended diagnostic tool for differentiation of a non-vascular from vascular etiology in patients with leg swelling.
Keywords: Lower extremity; Doppler ultrasound; Vascular disease
중심 단어: 하지; 도플러 초음파; 혈관 질환
서 론
하지부종을 보이는 환자에서 그 원인은 매우 다양하다[ 1, 2]. 내과적인 기저 질환이 원인인 경우도 있지만 혈관 질환이 원인인 경우 임상양상이 더 심각하고 중요한 질환일 가능성이 높다. 비혈관성 질환과 혈관성 질환의 원인 감별은 그 치료가 다르기 때문에 중요하다. 이런 이유로 하지부종 환자에서 혈관 초음파의 역할은 상당히 중요하다고 할 수 있다. 원인을 알 수 없는 하지부종 환자에서 혈관 초음파를 시행할 경우 혈관 질환이 원인인 비율이 높게 보고되었으며, 림프스캔 검사를 같이 시행하면 약 70%까지 혈관성 질환으로 인한 하지부종을 진단하였다는 보고도 있다[ 3]. 본 종설에서는 하지부종을 보이는 환자에서 흔한 혈관성 질환의 원인을 알아보고 혈관 초음파의 유용성과 실제 적용에 관해서 알아보고자 한다.
본 론
하지부종의 원인
혈관성 질환
편측 하지부종을 초래하는 원인으로 만성 정맥부전, 심부정맥 혈전증, 림프부종, 장골정맥 압박 증후군(iliac vein compression syndrome), 슬와동맥류(popliteal aneurysm), 혈관재개통술 후 상태(post-revascularization), 혈관 기형(Klippel-Trenaunay syndrome, Parkes-Weber syndrome 등), 구획 증후군(compartment syndrome) 등이 있다. 양측 하지부종을 일으킬 수 있는 원인으로는 악성종양, 혈관성 중심정맥 고혈압(대정맥 폐색, 대정맥 혈관기형), capillary leak syndromes (쇼크, 화상 손상) 등이 있다.
비혈관성 질환
편측 하지부종의 경우, 감염증/염증(봉와직염, 골수염, 농양), 외상, 종아리 근육 위축, 슬와낭종, 악성종양/림프종, 신경성 원인(복합부위 통증 증후군[chronic regional pain syndrome]), 신경병증, Charcot foot, 후복막 섬유화증(retroperitoneal fibrosis), 인위적인 다리 부종(factitial limb swelling) 등의 원인들이 있다[ 1]. 양측 하지부종의 원인으로, 심부전, 비혈관성 중심정맥고혈압(nonvascular central venous hypertension), 폐색성 수면무호흡증(obstructive sleep apnea), 폐고혈압, 만성 폐색성 폐질환, 가성부종(pseudoedema, lipedema), 비만, 약물, 임신, 만성 신부전, 간경화, 단백질 결핍, 호르몬 불균형(Cushing’s syndrome, 스테로이드 투여, 갑상선기능저하/항진증), 특발성 부종(idiopathic [cyclic] edema) 등이 있다[ 2].
병력에 의한 하지부종의 감별
하지부종의 발생이 급성인지 만성인지의 여부, 편측성인지 양측성인지의 여부, 악화 요인이나 호전 요인이 있는지의 여부, 동반된 피부 소견 등이 있는지의 여부가 원인 감별에 매우 중요한 요소가 될 수 있으며, 이 외에도 기저 내과적 질환의 여부, 사회적인 활동 형태나 직업의 종류 등도 원인 파악에 도움을 줄 수 있다.
혈관성 질환이 원인인 경우, 편측성으로 급성 혹은 만성적인 경과를 보이며 다양한 피부 소견을 이차적으로 동반하는 경우가 많다. 한 보고에 의하면 약 1/3의 환자에서 피부 병변이 동반된다고 한다. 내과적 질환 등 비혈관성 질환의 원인인 경우에는 대개는 양측성, 만성적인 양상을 보이며, 심부전, 신부전, 만성 간질환, 심한 영양 결핍 상태(저알부민혈증이 흔히 동반), 오랜 기간의 침상 생활 등의 원인이 있다.
약물도 흔한 하지부종의 원인이 된다. 혈관확장제(hydralazine, minoxidil, dihydropyridine, calcium channel blockers, and alpha blockers)가 흔한 원인이며, nonsteroidal anti-inflammatory drugs, thiazolidinediones, insulins, estrogens, progestins, androgens, aromatase inhibitors, tamoxifen 등은 나트륨 저류효과로 하지부종을 유발한다. 이 외에도 항전간제(gabapentin, pregabalin), 항암 약제(cisplatin), 항우울제, 도파민 작용제(pramipexole, ropinirole) 등의 약물들도 하지부종을 일으키나 그 기전은 불확실하다[ 1]. 동맥 질환의 경우 대개는 하지부종을 유발하지 않으며, 대부분 정맥 질환에 의해 발생하며, 림프부종의 경우에도 하지부종을 유발할 수 있다. 궤양이 동반된 경우에는 동맥 질환에 의한 경우가 더 많으므로 추가적인 평가가 필요하다.
신체 진찰 소견에 의한 하지부종의 감별
신체 진찰 소견은 하지부종을 보이는 환자에서 원인 감별을 위해 매우 중요한 역할을 한다. 부종의 양상, 이차적인 피부 변화 소견의 여부, 궤양의 여부 등이 주요 감별점이다( Figs. 1- 3).
전신 질환에 의한 하지부종
대개는 내과적인 질환을 동반하고 있으며, 양측성, 만성적으로 발생하는 경우가 많다. 특히 무릎 이하의 양측 하지에 함요부종(pitting edema) 소견을 보이며, 이차적인 피부 변화 소견은 드물다.
만성 정맥부전, 하지 정맥류
만성적인 정맥 내 판막 기능의 이상으로 유발되는 만성 정맥부전은 대개 편측의 하지부종을 유발하며, 이차적인 피부 변화 소견이 흔히 동반된다. 지렁이처럼 꾸불꾸불한 정맥혈관이 육안적으로 확장되어 있는 경우 하지 정맥류라 지칭하며 특히 중년 여성에게서 흔히 발병한다. 동반되는 이차 피부 변화로는 telangiectasia, reticular vein, hyperpigmentation, eczema, atrophic blanche, lipodermatosclerosis, corona phlebectatica 등이 있으며, 진행된 경우 하지 궤양까지도 보일 수 있다( Fig. 1) [ 4].
심부정맥혈전증
대개는 급성의 양상으로 편측성 하지부종을 보이며, 때로는 phlegmasia cerulea dolens의 응급 상황을 보이기도 한다( Fig. 2).
림프부종
만성적인 경과를 보이며 특징적인 소견을 보인다( Fig. 3). 발등이 두툼하게 올라오는 소위 ‘buffalo hump’ 소견을 보일 수 있고, 발가락이 깍두기 모양처럼 변하는 ‘squared toe’ 양상을 보이며, 발가락 피부를 꼬집듯이 잡아 올려도 당겨지지 않는 ‘Stemmer sign’을 보일 수도 있다[ 1].
하지부종 환자에서 혈관 초음파의 적용
혈관 초음파 검사는 일반 초음파와는 달리 혈류의 존재 유무, 혈역학적인 정보를 얻을 수 있다는 점에서 많은 초음파 지침에서 하지부종 환자의 감별 진단 검사로 이용할 것을 권고하고 있다[ 5, 6]. 초음파 모드는 B-mode (gray scale mode), color flow Doppler mode, Spectral Doppler mode 모두를 적용하여 검사를 시행한다[ 7]. 대개 5-7.5 MHz 주파수의 탐촉자를 이용하여 검사를 하나 비만인 환자나 하지부종이 매우 심한 경우 3-5 MHz 주파수 탐촉자를 사용하기도 한다. 대부분의 경우 누운 자세로 검사를 하지만, 만성 정맥부전이나 하지 정맥류가 의심되는 경우 선 자세로 하거나, 누운 상태에서 reverse Trendelenburg (머리를 올린 상태) 자세로 검사를 시행한다. 다리는 바깥쪽으로 돌리고 무릎을 약간 굽힌 자세를 취한다. 먼저 B-mode 검사를 시행하여 해부학적 정보를 얻게 되며, 다음으로 도플러 검사를 시행하여 혈류의 존재 여부나 혈역학적 정보를 획득한다( Table 1).
초음파 소견에 의한 하지부종의 감별
혈관 질환성 하지부종
대부분 만성 정맥부전(하지 정맥류 포함), 심부정맥혈전증 등이 원인인 경우가 많다. 또한 림프부종이 원인인 경우도 있지만, 이 경우 초음파의 진단적 역할은 매우 미미하며 림프스캔 같은 확진 검사가 필요하다. 동맥 질환에 의해서도 하지부종은 발생할 수 있다.
만성 정맥부전, 하지 정맥류
B-mode 초음파에서 대복재 정맥이나 소복재 정맥의 직경이 확장되어 있는 경우가 많고, 원위부를 압박하면서 Spectral 도플러 초음파 검사를 시행하였을 때 대복재 정맥이나 소복재 정맥 부위의 역류 소견을 관찰할 수 있다( Fig. 4). 0.5초 이상의 역류 소견이 있을 경우 양성으로 판정한다. 슬와정맥이나 대퇴정맥 등의 심부정맥에 대한 초음파 역류 기준은 1초 이상일 경우 양성으로 판정한다.
심부정맥혈전증
B-mode 초음파에서 정맥 내 혈전이 관찰된다( Fig. 5). 압박 테스트를 시행하였을 때 압박이 잘 되지 않거나 전혀 되지 않는 것을 관찰할 수 있으며( Fig. 6), 판막의 움직임이 고정되어 있다. Color mode 초음파에서는 부분적으로 혹은 전체적으로 혈류 결손 소견을 볼 수 있다( Fig. 7). Spectral mode에서는 혈류가 증강(augmentation)되는 소견이 없고, 호흡에 따른 자발성(spontaneity), 위상(phasicity)이 보이지 않으며, 부분 폐색인 경우 monotonous wave pattern을 보이고, 완전 폐색이 있는 경우 정맥 파형이 소실된다( Fig. 8) [ 7].
림프부종
전형적으로 간질 내 부종 소견을 보인다( Fig. 9). 때때로 정맥 내 역류 소견이 동반되는 경우(lymphovenous insufficiency)도 있으므로 정맥 검사도 같이 시행하는 것이 권고된다.
장골정맥 압박 증후군(iliac vein compression syndrome)
장골정맥의 해부학적인 특징으로 유발되는 혈관 압박 증후군으로서 좌측의 총장골정맥이 척추뼈와 우측의 총장골동맥에 의해 압박되어 발생한다[ 8]. 이러한 이유로 하지부종은 좌측에서 주로 발생하며 정맥 내 혈전증을 동반하므로 혈관 초음파 검사로 진단할 수 있다. 혈전증이 동반하지 않는 경우나, 환자가 비만인 경우에는 초음파 검사가 제한적일 수 있으며 이때는 컴퓨터단층촬영 검사를 시행하면 진단에 도움을 줄 수 있다( Fig. 10).
슬와동맥류(popliteal aneurysm)
일종의 혈관 압박 증후군으로서 슬와정맥을 압박하여 하지부종을 초래할 수 있다.
비혈관성 하지부종
봉와직염
염증이나 감염증은 하지부종을 유발하는 흔한 비혈관성 원인이다. 전형적으로 간질부종을 보인다. 때로는 봉와직염의 원인이 되는 숨어 있는 농양 소견이 관찰되기도 한다[ 9].
베이커 낭종(Baker’s cyst)
무릎 뒤쪽 슬와부위의 종창이 보이며 초음파에서는 혈관을 압박하는 낭종성 병변이 관찰된다. 파열된 경우 갑자기 발생하는 종아리의 통증과 부종 등의 급성기 양상을 보인다[ 10].
하지부종 환자에서 초음파 진단 알고리즘
임상적으로 특히 심부정맥혈전증이 의심되는 경우 초음파 검사를 고려해야 하는데 임상 척도로 대개 Wells score를 이용한다. Wells score가 2점 미만인 경우 심부정맥혈전증의 저위험군으로 여겨 D-dimer 검사를 먼저 시행한 후 양성인 경우 초음파 검사를 시행할 수 있고, 2점 이상인 경우 고위험군으로 생각하여 혈관 초음파 검사를 먼저 시행할 수 있다( Fig. 11) [ 10].
결 론
하지부종 환자에서 그 원인은 매우 다양하며, 특히 혈관성 질환으로 인한 경우 임상적으로 치료가 시급한 경우가 많다. 전신 질환 등 비혈관성 질환과의 감별이 중요하며, 이런 환자들에서 혈관 초음파를 적극적으로 활용하는 것이 정확한 진단 및 초기에 적절한 치료 방침을 결정하는 데 있어 중요한 역할을 할 수 있으며, 하지부종을 보이는 환자에서 반드시 시행하여야 할 진단 도구로 고려해야한다.
Figure 1.
Chronic venous insufficiency. (A) Chronic venous insufficiency with varicose vein. Left leg shows swelling below the knee and typical ‘champagne bottle leg’ appearance with secondary skin changes. Both legs show varicose of great saphenous vein. (B) Chronic venous insufficiency with secondary skin changes. Especially at the ankle, there are various skin changes including hyperpigmentation, atrophic blanche, and lipodermatosclerosis. (C) Chronic venous insufficiency with secondary skin changes. This ‘corona phlebectatica’ finding predicts disease severity indicating high probability of venous ulceration in the future. 
Figure 2.
This patient shows abrupt onset of burst-like swelling, pain, and redness of the right leg. This ‘phlegmasia cerulea dolens’ finding requires urgent or emergent treatment such as catheter-directed thrombolysis, mechanical thrombectomy, or surgical open thrombectomy. 
Figure 3.
Right leg shows typical lymphedema appearance of findings with squared toe appearance, buffalo hump, and elephantiasis-like skin change. 
Figure 4.
Chronic venous insufficiency. (A) Doppler ultrasound shows venous reflux longer than 1 second in the great saphenous vein at the thigh level (in the patient from Fig. 1). (B) Doppler ultrasound shows venous reflux longer than 1 second in the great saphenous vein below the knee (in the patient from Fig. 1). BK, below knee; AC, angle correction. 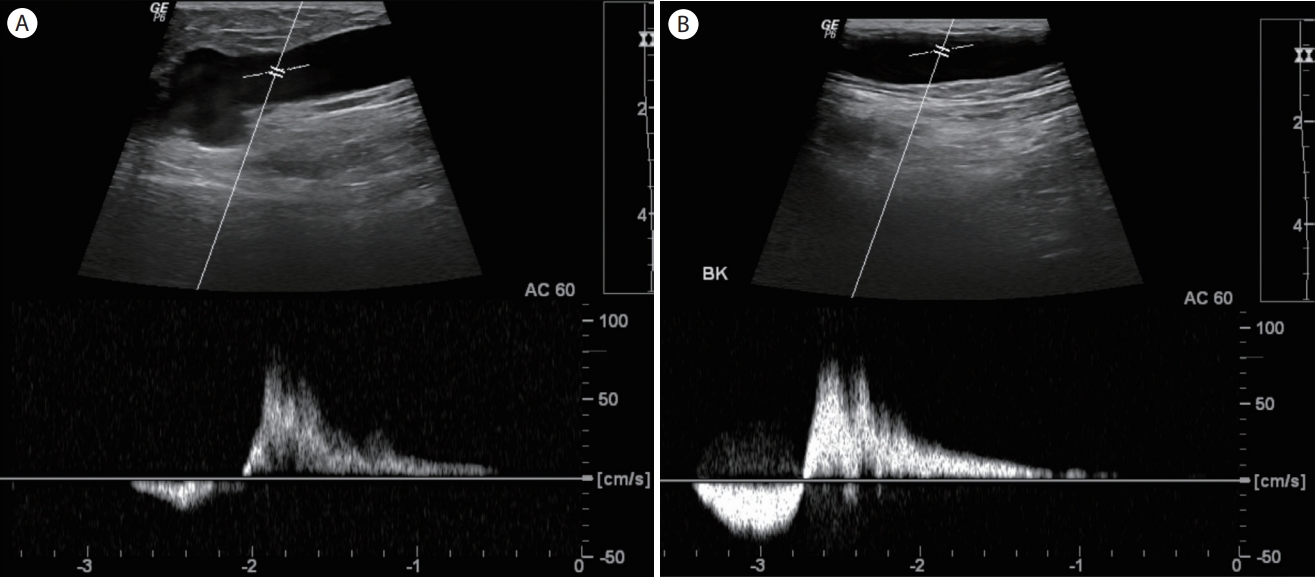
Figure 5.
In a patient with deep vein thrombosis, B-mode Doppler ultrasound shows an echogenic thrombus within the common femoral vein. 
Figure 6.
In a patient with deep vein thrombosis, the common femoral vein cannot be compressed due to thrombosis on B-mode Doppler ultrasound (positive compression test). LT, left; CFV, common femoral vein; COMP, compression; THR, thrombus. 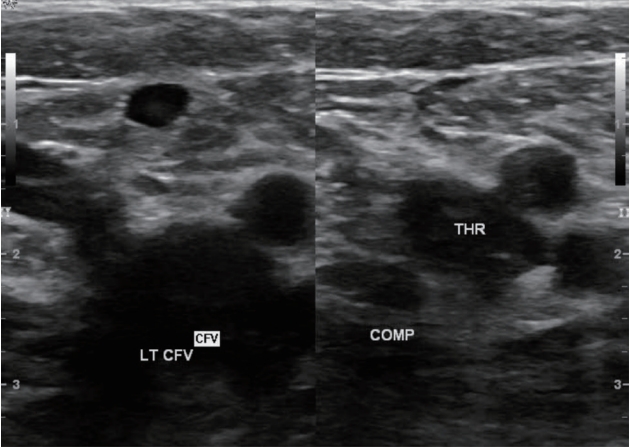
Figure 7.
In a patient with deep vein thrombosis, color flow Doppler ultrasound shows a filling defect due to thrombus. 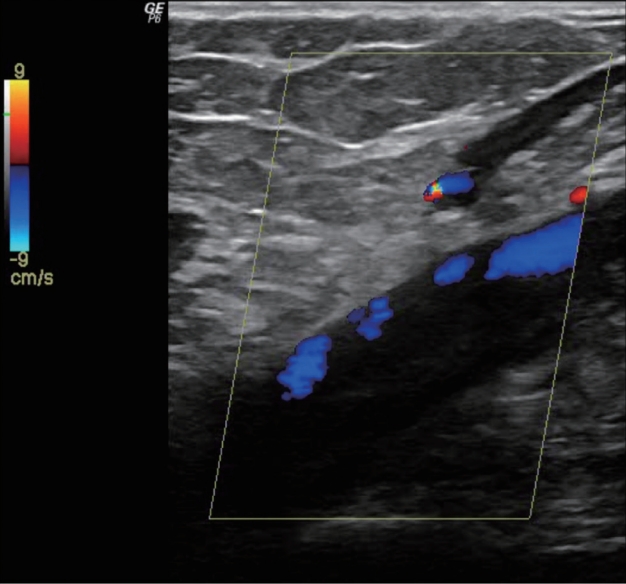
Figure 8.
Spectral Doppler ultrasound shows a monophasic wave pattern without phasicity in partial deep vein thrombosis. CFV, common femoral vein; LT, left; AC, angle correction. 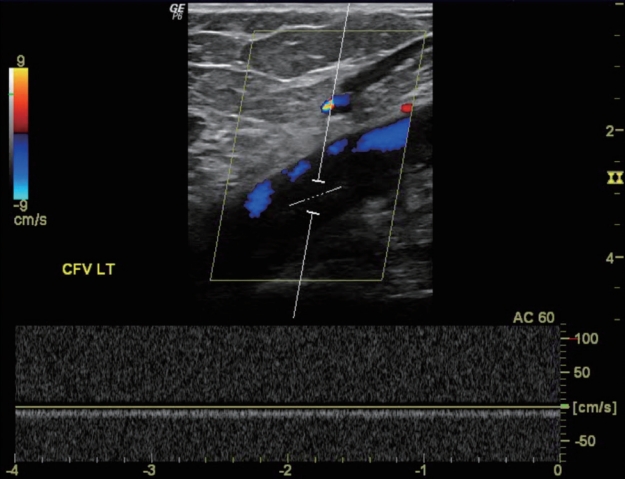
Figure 9.
Gray scale ultrasound shows moderate interstitial edema at the ankle (ANK) in a patient with lymphedema. 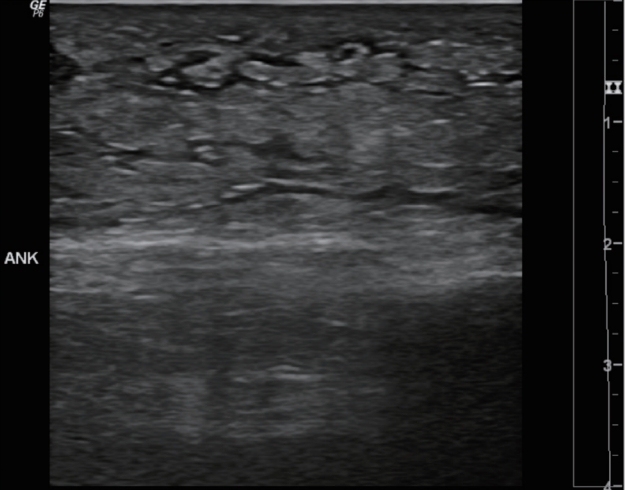
Figure 10.
May-Thurner syndrome. (A) Computed tomography (CT) scan shows compression of the left common iliac vein (CIV) between the right common iliac artery (CIA) and vertebral body. There is a thrombus within the left CIV. (B) CT scan shows a thrombus within the left external iliac vein (EIV). (C) CT scan shows the thrombus within the left femoral vein (FV) with marked swelling of the left leg (at the mid-thigh level). SFA, superficial femoral artery. 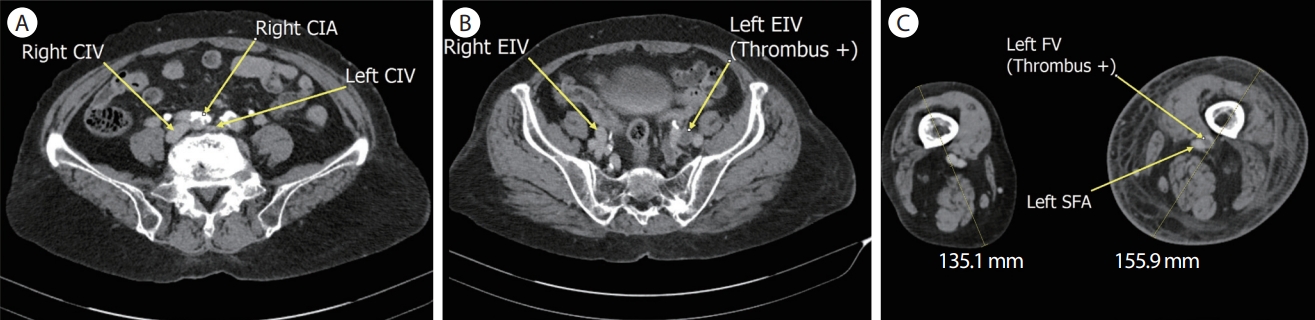
Figure 11.
Clinical decision algorithm for deep vein thrombosis (DVT) suspicion in a patient with leg swelling. Modified from reference [ 10]. US, ultrasonography; NPV, negative predictive value. aWells score < 2; bWells score ≥ 2. 
Table 1.
Interpretation criteria of venous Duplex imaging [ 7]
|
Gray scale/compression |
Color Doppler |
Doppler signal |
|
Normal |
No intraluminal echoes, free of echogenic material |
Color fills entire lumen |
Spontaneous, phasic, and augments with distal compression |
|
Vein fully coapts with external compression |
|
Abnormal: partially occlusive thrombus |
Vein lumen partially filled with echoes |
Defect in color as it is displayed around thrombus may appear normal if thrombus is small or color Doppler scale, and gain settings are inappropriate |
May be normal or abnormal (see below for abnormal) |
|
Vein partially coapts with external compression |
|
Abnormal: totally occlusive thrombus |
Vein filled with intraluminal echoes (veins may appear normal in circumstances of acute thrombus) |
Absence of color |
Absence of spectral Doppler signal, continuous signal, absent or reduced phasicity and the lack of pulsatility in certain upper extremity and central veins |
|
Vein does not coapt with external compression |
REFERENCES
1. Fish III JH, Lurie F. Evaluation of edema of the extremity. In: Chaar CO, ed, ed. Current management of venous diseases. 1st ed. New York: Springer, 2018:51–63.
2. Seller RH, Symons AB. Differential diagnosis of common complaints. 7th ed. Philadelphia: Elsevier, 2018.
4. Lurie F, Passman M, Meisner M, et al. The 2020 update of the CEAP classification system and reporting standards. J Vasc Surg Venous Lymphat Disord 2020;8:342–352.   5. AIUM practice parameter for the performance of a peripheral venous ultrasound examination. J Ultrasound Med 2020;39:E49–E56. 6. Gillespie D, Glass C. Importance of ultrasound evaluation in the diagnosis of venous insufficiency: guidelines and techniques. Semin Vasc Surg 2010;23:85–89. 7. Volz KR. Peripheral venous evaluation. In: Hagen-Ansert SL, ed, ed. Textbook of diagnostic sonography. 1st ed. Philadelphia: Elsevier, 2018:1025–1047.
9. Pellerito JS. Nonvascular findings encountered during venous sonography. Pellerito JS, Polak JF. Introduction to vascular ultrasonography. 6th ed. Philadelphia: Elsevier, 2020:483–493.
10. Wittens CHA, Strijkers RHW. The acutely swollen leg. In: Loftus I, Hinchliffe RJ, ed, ed. Vascular and endovascular surgery: a companion to specialist surgical practice. 6th ed. Philadelphia: Elsevier, 2019:301–311.
|
|