원발성 복막수염에 의한 급성복증으로 시행한 초음파에서 우연히 발견된 대장암 증례
요약
원발성 복막수염에서는 대부분 인접 대장벽의 이상을 동반하지 않으나 간혹 대장벽 비후를 동반하는 경우도 있다고 한다. 급성 복통이 호전되고 원발성 복막수염이 회복된 뒤에도 대장벽 비후가 지속되면 대장 내시경 검사와 같은 추가적인 검사가 필요하겠다. 저자들은 급성 복통으로 내원하여 초음파 검사에서 원발성 복막수염으로 진단된 환자에서 대장벽 비후가 동반되었을 때 원발성 복막수염이 좋아지고, 복통이 없어진 후에도 대장벽 비후가 지속되어 그 원인을 규명하기 위하여 대장 내시경 검사 및 조직 검사로서 대장암으로 진단된 증례를 보고하는 바이다.
중심 단어: 급성복증; 초음파; 원발성 복막수염; 대장암
Abstract
Acute abdomen is mainly caused by peptic ulcer perforation, cholecystitis, or appendicitis, diverticulitis. But recently epiploic appendagitis is increasing in incidence as a cause of acute abdomen due to the development of ultrasound and computed tomography. Epiploic appendagitis occurs primarily or secondarily. Primary epiploic appendagitis is a self-limiting disorder caused by an ischemic change of the appendage. It can mimic other causes of the acute abdomen such as appendicitis or diverticulitis. An adjacent colonic wall abnormality is nearly absent in primary epiploic appendagitis. Secondary epiploic appendagitis usually occurs due to inflammation of an adjacent organ due to appendicitis or diverticulitis. Secondary epiploic appendagitis caused by cancer is not reported yet. The authors report a case of a 64-year-old female patient who was incidentally diagnosed with colon cancer by ultrasound due to an acute abdomen caused by primary epiploic appendagitis.
Keywords: Acute abdomen; Ultrasound; Primary epiploic appendagitis; Colon cancer
서론
급성복증은 발병 후 24시간에서 2-3일 내에 적절한 치료를 해야 하는 질환의 통칭으로 주로 소화성 궤양에 의한 천공, 장폐쇄, 담낭염, 게실염, 충수염 등이 주된 원인이나[ 1] 최근 초음파와 복부 전산화단층촬영 등의 발달로 예전에는 진단이 어려웠던 복막수염이 증가하는 추세이다[ 2]. 복막수염은 원발성 복막수염과 속발성 복막수염으로 나눌 수 있다. 원발성 복막수염은 기저질환 없이 복막수의 염전, 혈전 등에 의한 허혈성 변화에 의해 발생하며, 인접한 대장에 이상이 없는 것이 일반적이다. 임상적으로는 국소적인 압통, 반발통이 특징적이며, 대부분 수일 이내 저절로 회복되나 간혹 수주간 지속되는 경우도 있다. 속발성 복막수염은 주변 장기의 염증에 의하여 생기며 주로 충수염, 게실염 등의 이차적인 세균 감염으로 생긴다[ 3, 4]. 대장암에 의한 속발성 복막수염의 증례는 아직 보고되어 있지 않다[ 5]. 저자들은 급성 복통으로 시행한 초음파 검사에서 원발성 복막수염에 동반된 층구조가 불명확한 장벽 비후의 원인을 찾기 위한 대장 내시경 및 조직 검사에서 진단된 구불결장-하행결장 이행부의 대장암을 경험하였기에 보고하는 바이다.
증례
64세 여자가 3일간의 좌하복부 불쾌감과 내원 당일 갑작스럽게 악화된 극심한 좌하복부 통증을 호소하며 내원하였다. 진찰상 좌하복부 압통과 반발통이 심하였고 통증은 국소적이었다. 복부 초음파 검사에서 좌하복부 장벽에 인접하여 타원형의 고에코 병변이 보였고, 층구조가 불명확한 장벽 비후와 액체저류가 관찰되었다( Fig. 1). 복막수염 진단하에 소염제 등의 치료 중증세의 호전이 없어 2일 후 시행한 추적 초음파 검사에서 타원형의 고에코 병변은 변화가 없었으나, 장벽 비후와 액체 저류가 심해져 복부 전산화단층촬영을 의뢰하였다. 검사 결과 액체 저류를 동반한 불규칙한 대장벽 비후가 있고 고밀도의 테두리를 가지는 저밀도의 타원형 종괴가 발견되어 복막수염으로 판독되었으나 일반적인 복막수염과 달리 불규칙한 대장벽 비후가 의심되어( Fig. 2) 항생제를 사용하였다. 또한 대장벽 비후의 원인을 알기 위하여 대장 내시경을 권유하였으나 통증이 너무 심하다고 환자가 거부하여 추가적으로 소염제와 항생제를 2주간 더 사용하였다. 그 후 복통은 거의 호전되었고 추적 초음파 검사 및 복부 전산화단층촬영에서 복막수염의 양상은 많이 호전되었으나, 층구조가 불명확한 대장벽 비후가 지속되어( Fig. 3 and 4) 시행한 대장 내시경 검사에서 구불결장-하행결장 이행부에 장관협착을 동반한 궤양성 종양이 있어 대장암을 의심하였고( Fig. 5) 조직 검사에서 고분화 선암으로 확진되었다.
고찰
급성복증의 원인 질환은 발병 부위에 따라 다르며 특히 하복부에 올 때는 충수염, 게실염 등이 주요 원인이며 복막수염은 드물었으나 최근 들어 초음파, 복부 전산화단층촬영 등 진단 기법의 발달로 복막수염이 급성복증의 원인으로 증가되는 추세이다[ 2]. 복막수염은 대장의 장측 복막에 달려 있는 복막수에 생기는 염증으로 원발성 복막수염과 속발성 복막수염으로 나눌 수 있다. 원발성 복막수염은 기저질환 없이 복막수에 국한된 염증으로 복막수의 염전, 혈전 등 허혈성 변화에 의해 발생하고, 좌하복부나 우하복부에 방사되지 않는 국소적인 통증을 호소하는 질환으로 대부분 수일 내에 호전되지만 10%에서는 수주간 지속될 수 있다[ 3, 4]. 간혹 원발성 복막수염을 게실염이나 충수염으로 오진하는 경우도 있다[ 5]. 속발성 복막수염은 주변 장기의 염증에 의해 생기며 게실염, 충수염, 담낭염 등의 이차적 세균 감염의 결과로 생긴다. 속발성 복막수염이 대장암과 연관된다는 증거는 아직 보고되지 않고 있다[ 6]. 원발성 복막수염에서 인접 대장벽에 이상이 없는 것이 대부분이지만 간혹 대장벽 비후를 동반하는 경우도 있다고 하며, 있더라도 경미하며 복막수염이 좋아지면 대장벽 비후도 없어지는 것이 보통이다[ 7]. 만약 이 증례처럼 원발성 복막수염에 의한 급성복증에서 대장벽 비후가 동반되었을 때, 급성 복통이 회복되고 복막수염이 좋아진 후에도 대장벽 비후가 없어지지 않는 경우 대장벽 비후의 원인에 대한 정밀 검사(대장 내시경 등)가 필요할 것으로 사료된다.
Figure 1.
(A) Gray-scale ultrasonography (3.5 MHz) shows bowel wall thickening with a loss of wall stratification (arrow). (B) Oval hyperechoic mass is seen adjacent to the bowel wall (arrow). Bowel wall thickening with a loss of wall stratification is also seen (arrowhead). (C) Linear probe (9 MHz) ultrasonography shows an oval hyperechoic mass with a hypoechoic rim. Color Doppler shows no blood flows within the mass (arrow). 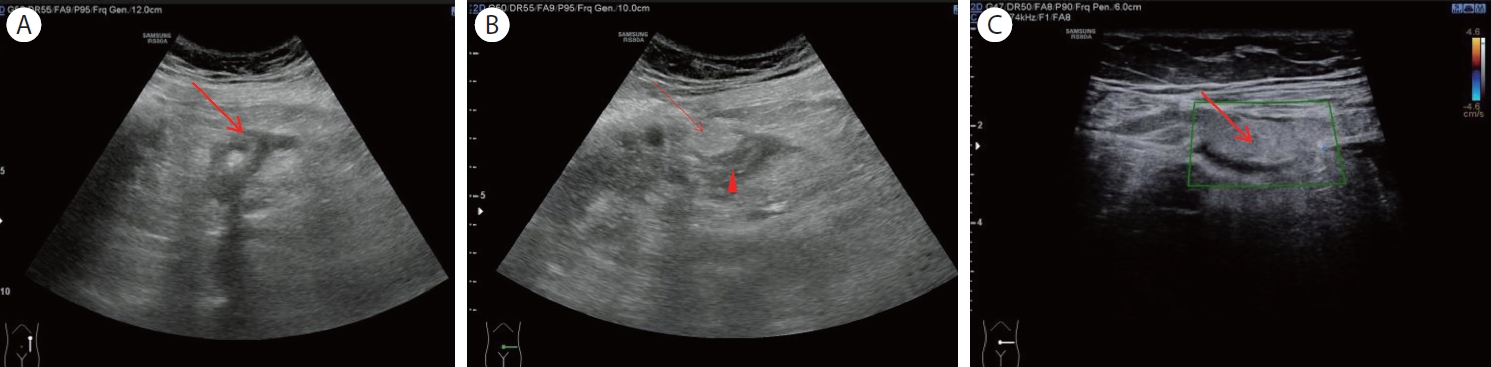
Figure 2.
(A) Gray-scale ultrasonography (3.5 MHz) shows aggravated bowel wall thickening with a loss of wall stratification compared with a previous examination (arrow). (B) Computed tomography shows irregular colon wall thickening with the fluid collection and also shows a hypodense oval mass with a hyperdense rim (arrow). 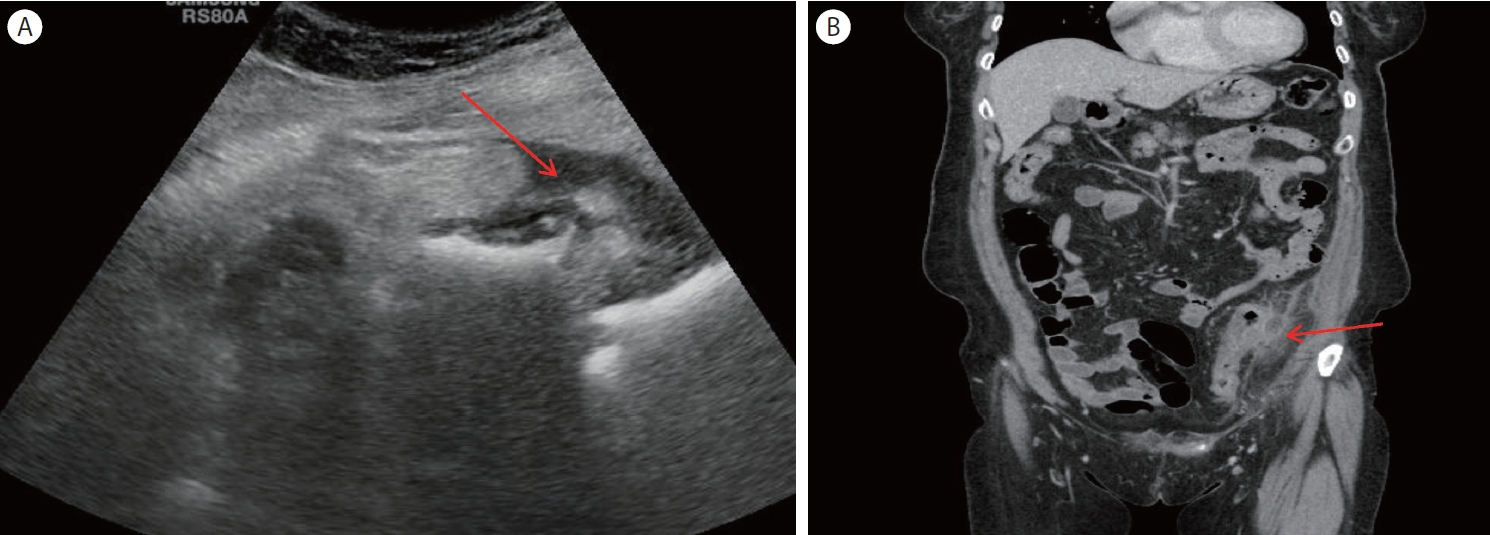
Figure 3.
(A, B) Gray-scale ultrasonography (3.5 MHz) shows an improved hyperechoic mass compared with a previous ultrasonographic examination, but bowel wall thickening with a loss of wall stratification persisted (arrows). 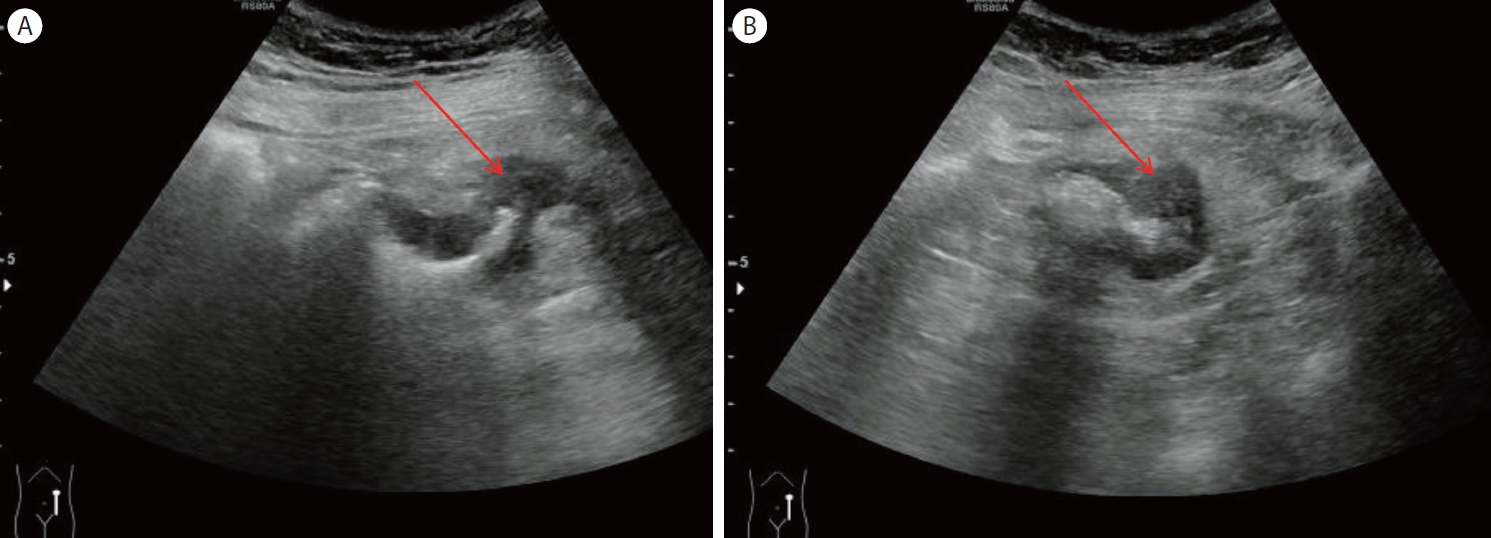
Figure 4.
(A, B) Gray-scale ultrasonography (A: transverse scan, B: longitudinal scan) show persistent bowel wall thickening with loss of wall stratification (arrows) and hyperechoic fat deposition around the thickened bowel wall (arrowhead). (C) Computed tomography shows persistent colonic wall thickening without signs of appendagitis (thick arrow). 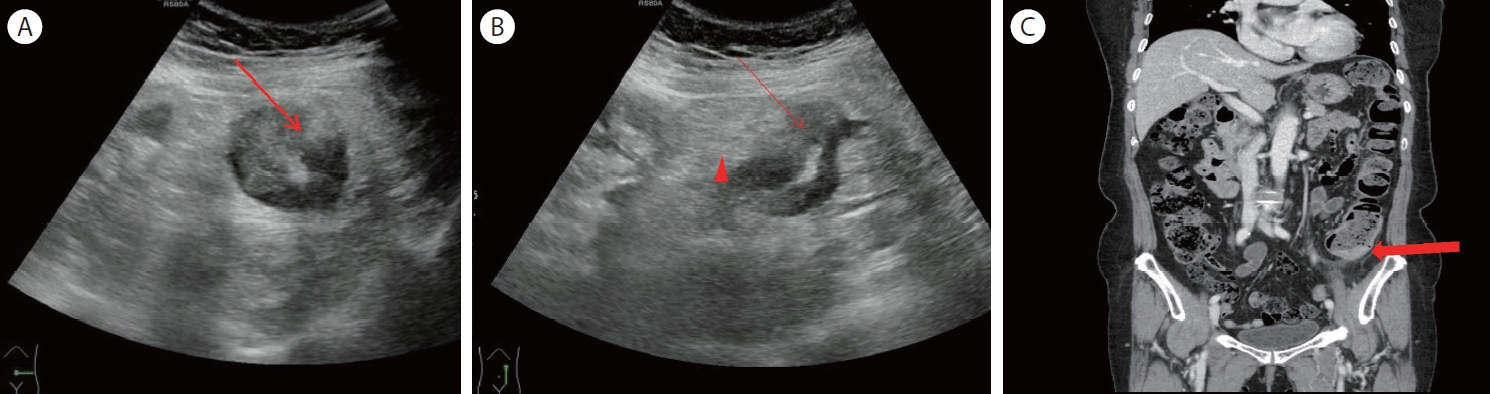
Figure 5.
Colonoscopic examination shows an ulcerating mass with luminal narrowing at the junction between the sigmoid colon and the descending colon which suggests colon cancer (arrow). 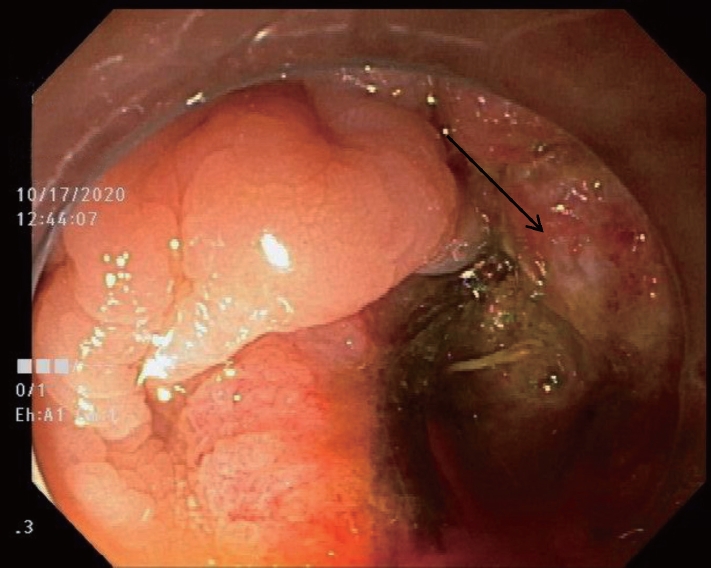
REFERENCES
1. Gans SL, Pols MA, Stoker J, Boermeester MA; expert steering
group. Guideline for the diagnostic pathway in patients with acute abdominal pain. Dig Surg 2015;32:23–31.   3. Kim DH. Ultrasound of digestive tract with case review. 1st ed. Seoul: Beom-mun edu, 2018.
4. Cho KH. Primary eppiploic appendagitis with adjacent colonic wall thickening. Clinical Ultrasound 2017;2:73–76.
6. Almeida AT, Melão L, Viamonte B, Cunha R, Pereira JM. Epiploic appendagitis: an entity frequently unknown to clinicians--diagnostic imaging, pitfalls, and look-alikes. AJR Am J Roentgenol 2009;193:1243–1251. 7. Singh AK, Gervais DA, Hahn PF, Sagar P, Mueller PR, Novelline RA. Acute epiploic appendagitis and its mimics. Radiographicsd 2005;25:1521–1534.
|
|