



서 론
포충증(hydatid disease, echinococcosis)이란 단방조충(Echinococcus granulosus) 혹은 다방조충(Echinoccocus multilocularis)의 유충의 감염으로 발생하는 질환을 말한다. 단방조충(Echinococcus gra nulosus)에 의한 감염은 cystic echinococcosis (CE)라 하고 질환의 경과가 느려 수년간 무증상으로 지내는 경우가 많다. 이에 반해 다방조충(Echinoccocus multilocularis)에 의한 감염은 alveolar echinococcosis라 부르며 더 드물게 발생하지만 빠르게 진행하고, 예후가 좋지 않다[1]. 인체에서는 간이 가장 흔히 침범되는 장기(50-60%)이지만, 폐(10-30%), 비장, 신장, 뇌 등 인체 어느 부위도 침범될 수 있다[2].
포충증은 인수공통질환(zoonosis)으로서 개나 늑대 등이 종숙주이고 사람이나 양, 염소, 돼지 등이 중간숙주이다[3]. 전 세계적으로는 목축업을 하는 지역에 흔하여 아프리카, 남아메리카, 중동 지역 및 과거 소비에트 연방 지역 등에서 호발하지만, 국내에서는 매우 드문 질환이다[4]. 그러나 유행 지역에서 입국한 외국인 노동자의 국내 취업이 늘어나고, 해당 지역으로의 여행자가 늘어남에 따라 포충증의 빈도가 증가할 가능성이 높아, 포충증에 대한 관심과 이해가 필요할 것으로 생각된다. 본 종설에서는 가장 흔하게 발생하는 단방조충(E. granulosus)에 의한 간 포충증(hepatic hydatid disease, hepatic echinococcosis)의 진단과 치료에 대해 알아보고자 한다.
본 론
단방조충(E. granulosus)의 생활사(life cycle)
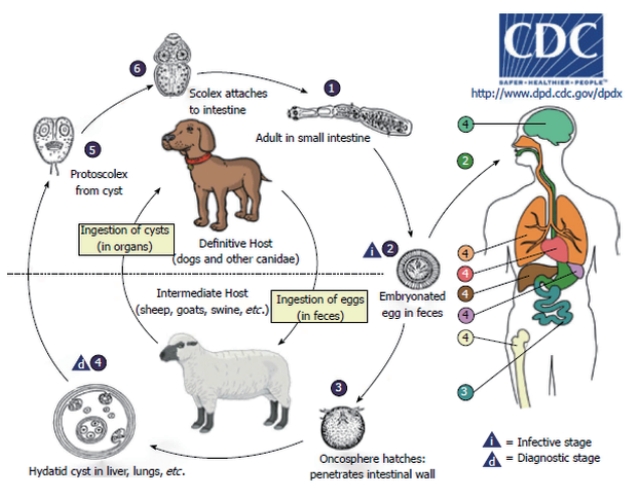
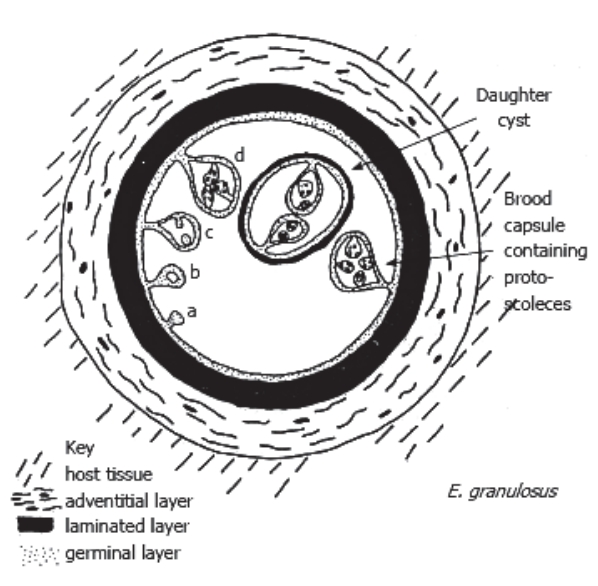
단방조충의 종숙주는 개, 여우 등이며, 중간숙주는 양, 소, 돼지 등이고, 사람은 우연숙주이다. 종숙주에 기생하는 단방조충(E. granulosus)의 성충에서 배출된 충란이 중간숙주에게 먹히면, 육구자충(oncosphere larva)으로 부화된 후 장벽을 뚫고 혈류나 림프계를 타고 간이나 다른 장기로 이동하여 조충유충(metacetodes)으로 진화하여 포충낭(hydatid cyst)을 만든다[5] (Fig. 1). 포충낭은 내포(endocyst)와 육아종성 숙주 반응(granulomatous host reaction)으로 인해 만들어진 내포를 둘러싸고 있는 숙주세포(pericyst or adventitia)로 이루어져 있다. 내포(endocyst)는 구형의 액체로 채워진 소낭(vesicle)으로서, 여러 개의 무세포층으로 구성되어 있는 외피층과 내부 세포층(종자층, germinal layer)으로 이루어져 있다. 내포의 내부 세포층에서 1차 번식포와 원두절(protoscolices)이 부화하고, 이어서 다양한 크기의 자낭포(daughter cyst)를 형성하기도 한다[5,6] (Fig. 2). 부화된 원두절(protoscolices)은 종숙주에 먹히면 부화되어 성충으로 자라게 된다(Fig. 1).
감염 경과 및 임상 양상(clinical manifestation)
낭포는 일반적으로 1년에 1-5 mm의 속도로 천천히 자라기 때문에 대부분의 사람들은 감염 후 오랜 기간 동안 무증상으로 지낸다. 따라서 증상은 대부분 성인이 되어서 나타난다[3,7,8]. 가장 흔한 증상은 우상복부 불편감이나 식욕부진이며, 촉진 시간비대나 종괴가 촉지될 수 있다. 그러나 낭포 크기의 증가로 인한 복통, 낭포 파열로 인한 아나필락시스(anaphylaxis) 반응, 자낭포의 담관 폐쇄로 인한 담관염 증상, 문맥 고혈압, 복수, 낭포의 2차 세균 감염, 포충낭 내 또는 횡격막하 농양 등이 합병증으로 발생할 수 있다[3,7,9,10]. 포충증의 90%에서 낭포는 담관과 연결되어 담관염 등의 증상을 일으키지만[6], 10%에서는 복강 내 파열로 인하여 아나필락시스나 2차 포충증을 일으킬 수 있다[3,10].
진단(diagnosis)
단방조충에 감염된 초기에는 대부분의 사람에서 증상이 없으므로, 우연히 발견되는 경우가 많다. 진단은 영상검사와 면역혈청학적 진단을 이용한다[1].
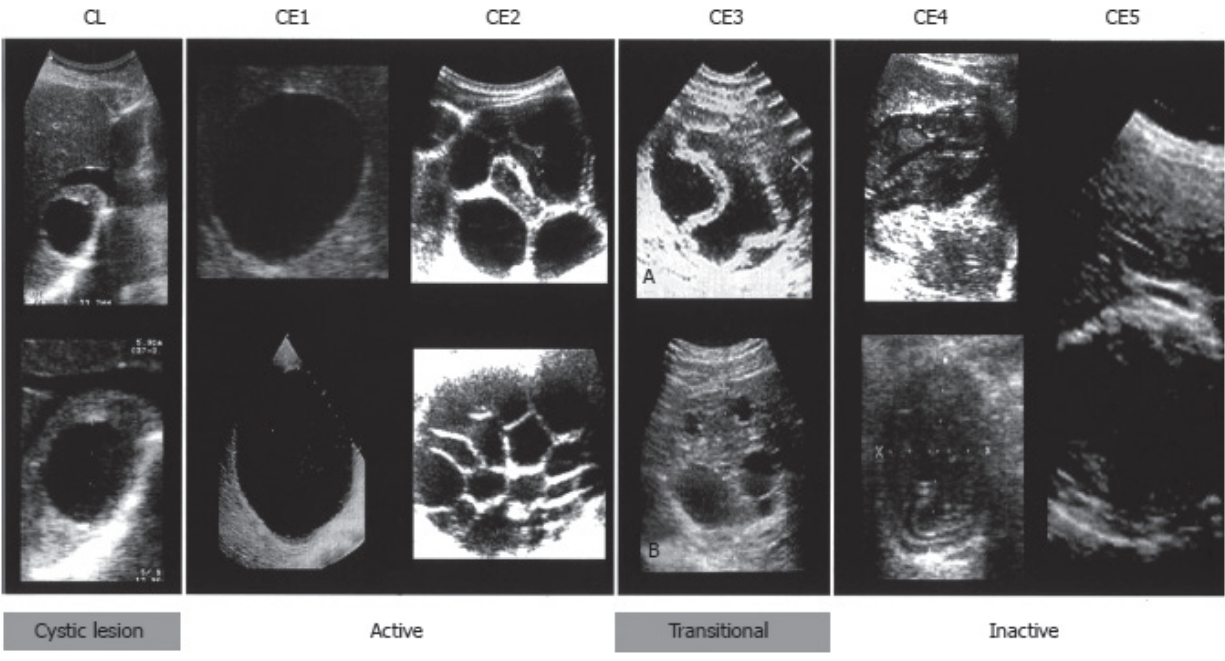
복부 초음파는 낭포의 위치, 수, 크기 및 활력(vitality)을 비교적 쉽게 평가할 수 있어 가장 많이 사용되는 영상검사이다[1]. 간 포충증의 초음파 분류는 1981년 Gharbi 등[11]이 처음 제안하였고, 2003년에는 World Health Organization (WHO)에서 새로운 분류 체계를 발표하였다[12] (Table 1). 이 분류 체계에서는 간 포충증으로 확진되기 전까지 검사가 더 필요한 단계를 cystic lesion으로 따로 분류하였다. 또한 CE는 활동기(active stage)인 CE1, CE2와 과도기(transitional stage)인 CE3, 그리고 비활동기(inactive stage)인 CE4, CE5로 분류하였다(Fig. 3). 최근 WHO 분류 체계의 수정 사항에 따르면, 석회화가 CE5 단계에만 있는 것이 아니고, 모든 단계의 포충증에서 존재할 수 있으므로 석회화의 존재가 포충낭의 비활성을 반드시 의미하는 것은 아니라고 밝히고 있다[13]. 최근 몇몇 연구에 따르면 CE3a (detached endocysts)는 과도기(transitional stage)이지만, CE3b (predominantly solid with daughter vesicles)는 활동기(active stage)에 속한다고 보고하였다[14,15].
복부 초음파 이외에 사용되는 영상검사로는 복부 computed tomography (CT) 및 magnetic resonance imaging (MRI)이 있으며, 1) 환자가 비만이거나, 포충낭이 횡경막 하부에 위치하는 등의 원인으로 인해 포충낭이 복부 초음파에서 보이지 않을 경우, 2) 포충낭의 위치가 복강 내 이외에 있는 경우, 3) 파종성(disseminated) 질환인 경우, 4) 포충낭의 합병증(infection, cysto-biliary fistulae 등)이 발생한 경우, 5) 수술 전후 평가 등의 경우에 이용된다. 특히 복부 MRI는 포낭 실질 내 액체 영역을 더 잘 평가할 수 있어 CT보다 선호되고 수술 전 평가에도 중요하다[7].
ELISA와 immunoblotting을 이용한 면역혈청학적 진단은 E. granulosus 의 포충낭액 항원 B (AgB)와 항원 5 (Ag5)를 이용하여 이루어진다. 그러나 이러한 면역혈청학적 진단은 민감도와 특이도가 낮고, 기술적 표준화가 아직 이루어지지 않았으며, 다른 기생충 항원(E. multilocularis, Taenia solium cysticercosis, schistosomiasis, liver flukes)과의 교차 반응이 있다는 단점이 있어 영상검사에 보조적으로 사용된다[7]. 또한 면역혈청학적 검사는 포충낭의 단계에 따라서도 양성률이 다른데, CE1과 CE4-CE5에서는 각각 30-58%, 50-87%에서 검사 결과 음성이며, CE2와 CE3에서는 5-20%에서 음성을 보인다. 또한 수술로 완전 절제가 이루어진 포충증의 경우에도 10년 이상 지속적으로 양성 결과를 보일 수 있어, 검사 결과 해석에 주의가 필요하다[16,17].
만약 간 포충증이 의심되는 환자에서 간의 병변이 종양이나 간농양 등과의 감별이 어렵고, 면역혈청학적 검사 결과 음성인 경우에는 초음파유도 미세바늘 천자(ultrasonography-guided fine needle aspiration)를 시행하여 흡인 낭액에서 원두절(protoscolices)이나 포충막(cyst membrane), 단방조충 항원 혹은 DNA를 발견하면 확진할 수 있다. 바늘 천자를 할 때에는 아낙필락시스의 위험이 2.5%까지 보고되고 있으므로[18] 극심한 주의를 기울여야 하며, 예방을 위해 검사 전 4일부터 검사 후 한 달까지 albendazole을 복용해야 한다[19].
치료(treatment)
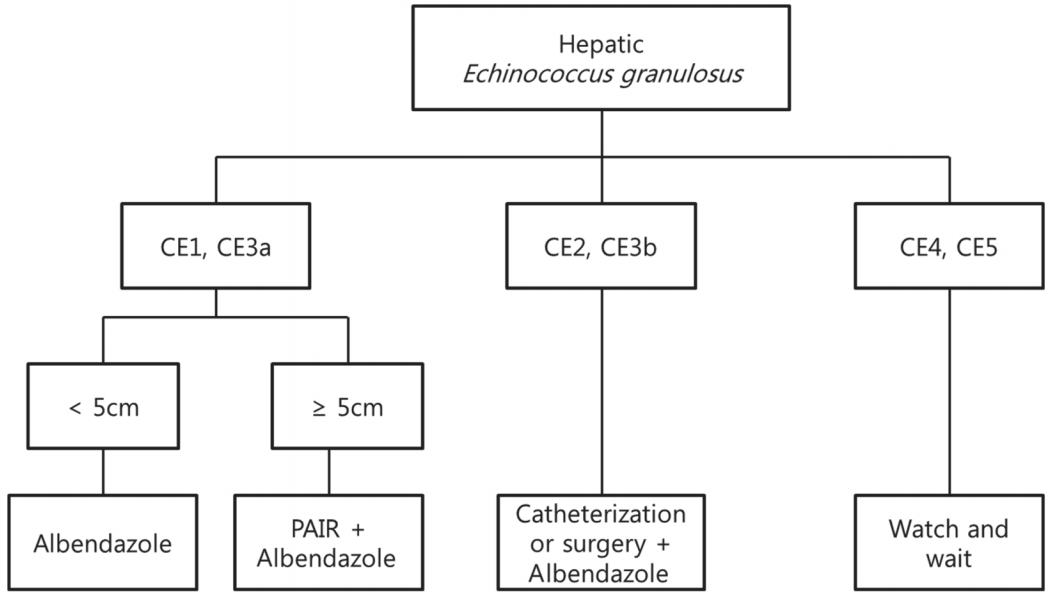
간 포충증의 치료로는 수술, 경피적 치료, 약물 치료의 세 가지 방법이 있다[20]. 현재까지 이 세 가지 치료법을 비교한 무작위 연구는 없어 명확한 치료 가이드라인은 없으므로, 간 포충증의 치료는 환자의 전신적 상태, 간 포충증의 상태, 가능한 치료 요건 등을 고려하여 이루어지게 된다[21]. 일반적으로 간 포충증의 치료 계획은 WHO 분류에 따라 세우게 된다. CE1과 CE3a에서 포충낭의 크기가 5 cm 미만인 경우에는 albendazole 단독 치료만으로 충분할 수 있으나, 5 cm 이상인 경우에는 경피적 치료인 “puncture, aspiration, injection of a scolecidal agent, and re-aspiration (PAIR)”과 albendazole 투여가 선호된다. CE2와 CE3b 포충낭의 경우에는 catheterization이나 수술적 제거가 필요하지만, CE4와 CE5의 비활성 포충낭의 경우에는 경과 관찰만으로도 충분할 수 있다(Fig. 4).
수술적 치료
다른 치료법의 발달로 인해 수술적 치료가 차지하는 비중이 줄고 있긴 하지만 합병증이 동반되어 있는 포충증(파열, 담관 분지와 연결된 포낭, 다른 장기의 압박, 감염, 출혈 등)이나 파열의 위험성이 높은 포낭, 혹은 수많은 자낭포(daughter cysts)로 인해 경피적 치료가 불가능한 경우에서는 수술적 치료가 필요하다[7]. 일반적으로, 아낙필락시스와 이차성 낭성 포충증 예방을 위해 수술 1주일 전부터 4주 후까지 albendazole 투여를 권장한다[20].
수술은 근치적 수술(radical surgery)과 보존적 수술(conservative surgery)이 있으며, 근치적 수술의 경우에는 포충낭 자체와 함께 주위낭벽(pericystic membrane)을 제거하며, 필요에 따라서 간 절제도 이루어진다. 보존적 수술에서는 포충낭 내부 내용물만 제거하고, 주위낭벽은 남긴 후 다른 방법(omentoplasty, capitonnage, or external drainage)을 이용하여 남은 부분(residual cavity)을 치료하는 방법이다[7]. 수술의 합병증은 3-25%이며, 재발률은 2-30% 정도로 알려져 있다[22-25].
경피적 치료
경피적 치료로는 PAIR와 catheterization technique이 있다. PAIR는 종자층(germinal membrane)을 scolicidal agent을 이용하여 파괴하는 방법으로, 1) 초음파를 이용한 포낭의 경피 천자(puncture), 2) 포낭액 흡인(aspiration), 3) scolicidal agent 주사(injection), 4) 액체 재흡인(re-aspiration)의 4단계로 이루어진다. Scolicial agent로는 hypertonic (15-20%) saline이나 95% ethanol이 가장 많이 사용된다[8]. PAIR는 보통 5 cm 이상의 CE1과 CE3a에서 사용되며, 석회화나 내부 고형 물질 등으로 인해 포낭 내부의 흡인이 불가능할 경우, 복강 내로 누출 위험성이 큰 경우, 혹은 담관과의 연결성이 의심되는 포낭의 경우는 금기증이다[1].
약물 치료
현재까지 포충증에 가장 흔히 사용되는 약물은 albendazole로서, 일반적으로 10-15 mg/kg/day 용량은 3-6개월 동안 투여한다. Albendazole을 사용할 수 없는 경우에는 mebendazole을 사용해 볼 수 있으나, 흡수가 albendazole에 비해 잘 되지 않으므로 더 높은 용량인 4 0-50 mg /kg /d ay가 필요하다[27]. Albendazole과 함께 praziquantel 40 mg/kg을 1주에 한 번 투여하는 경우, albendazole 단독보다 치료 효과가 더 좋다는 보고도 있다[28].
약물 치료 단독 사용은 5 cm 미만의 CE1, CE3a 포충낭에서 사용해 볼 수 있으며, 그 이외에는 수술이나 경피적 치료와 병합요법으로 사용된다[20]. 약물요법의 경우, 28.5-58% 정도의 완치율이 보고되고 있으며, 치료 기간을 연장한다 해도 완치율이 증가하지는 않는다[29-32].
약물요법의 일반적인 부작용으로는 두통, 구토, 호중구 감소, 탈모, 간독성 등이 있으므로 치료받는 환자에서는 정기적인 백혈구 및 간기능 검사가 필요하다. 간 부전, 임신, 골수부전 등은 치료의 금기이다[3].
결 론
간 포충증은 E. granulosus의 감염으로 인해 발생하는 질환으로, 성장 속도가 느려 종종 늦게 발견된다. 대부분 무증상인 경우가 많지만 우상복부 불편감, 담관염, 낭종 파열 및 아낙필락시스까지 일으킬 수 있다. 진단으로는 복부 초음파 및 혈청검사가 사용되며, WHO 분류가 치료 방법 선택에 이용된다. 치료 방법은 약물 치료, 경피적 치료 및 수술적 치료가 있다. 간 포충증은 국내에서는 매우 드문 질환이지만, 유행지역에서의 인구 유입 등으로 인하여 향후 그 빈도가 늘어날 것으로 예상되므로, 임상 경과, 진단, 및 치료에 대한 이해가 필요할 것으로 생각된다.